I believe that the primary educational material for medical education has gone through three phases. In the beginning was the medical text book. This was exemplified by Harrisons which rose to ascendancy not by being the first text book but by being the most innovative. Harrison unique innovation was arranging the sections by patient complaint rather than by disease. Here it is described in a fascinating history of the Harrison family of doctors:
PRINCIPLES OF INTERNAL MEDICINE would offer medical students a new way of approaching patients. The Cecil Textbook of Medicine, which had previously monopolized the American medical textbook market, took a less helpful approach. Its author, Russell Cecil, M.D., of Cornell Medical School in New York, had organized the textbook exclusively by disease, offering the definition, cause, symptoms and signs, methods of diagnosis, treatment, and prognosis for each one. This meant, of course, that a student must identify the patient's disease before the book would offer help. Principles of Internal Medicine, on the other hand, began with the patient. Tinsley [Harrison] devoted the first third of his textbook to symptoms and signs experienced by sick people, which included shortness of breath, swelling of the feet, and so on-leading from there to understanding the disease. The text mirrored the ideal practice of a physician. The first edition of his book, published in 1950, proved an instant and major success.

As good as UpToDate is it has some weaknesses. The EBM zealots take it to task for relying on expert opinion but I really don't have too much concern about that (my previous post on that took them to task for saying they are EBM when they are really an expert opinion source. That's why the list of author/editors is so important and impressive. They should be proud of what they are rather than claim to be EBM) .
What concerns me is UpToDate's inability to escape its CD-ROM DNA. I have been a subscriber to UpToDate since I was a resident and Burton Rose was still answering the phone to deal with bad CDs and pimping the still incomplete product in the hallways of Renal Week. The ascendancy of the Internet has allowed UpToDate to get out of the CD shipping business but they still refuse to link out even when it makes overwhelming sense. All of their articles are fully referenced, but not with links to the primary data or the pubmed reference but to an internal database record of the reference.

I get that isn't too hard to copy the PMID and drop it into google and that will pull the article, but why doesn't UpToDate just link-out?

This goes for other area where a link out makes sense. Here is a segment of UpToDates card on "Overview of the management of CKD in Adults"
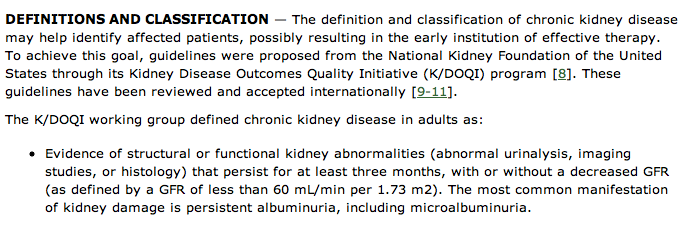
Wouldn't you expect, reference 8 to take you to the K/DOQI guidelines. They are free and available on the internet. UpToDate instead links to their internal reference of the AJKD supplement with the original publication of the K/DOQI guidelines, which are behind an Elsevier pay wall.

It feels that the editorial rules for UpToDate were created in the CD-ROM era of the 90's and haven't been updated for the internet era.
I beleive that, just as Harrison had an openning in the Internal Medicine textbook space by using patient oriented complaints to organize his text and Rose had an openning by using search and a unique editorial style, the technology of today provides a niche. I want an interactive textbook of medicine with comments, a Facebook "Like" button, a way to connect with other practitioners and share treatment pearls.
The renal fellow network and other knowledge focused medical blogs are early progenitors of this future but some pretty large problems need to be addressed:
- Organization. Blogs are reverse chronologic order by convention but given the random way that topics get posted, it makes for an unorganized structure. Solutions that are being used now include search and tags. Unfortunately, the tag clouds are so huge that they border on the useless. Search is good but a more structured table of contents and/or index would be great. I am delighted with the addition of the lecture and handout tabs on PBfluids, its a step that allows, at least me, to find things I have posted here before.
- Expiration of old data. Medicine is always evolving. Today's truth is tomorrow's MMR-autism fiasco. These medical blogs need a way to mark expired information as such. A perfect example is the ATN trial by the VA and NIH. Prior to that study I was firmly in the more dialysis for acute kidney injury camp. After that was published I marked my acute kidney injury lecture, as being pre-ATN trial. This meant something to me, but my readers likely had no idea what that meant. How many other educational resources were obsoleted by that medical about-face?
Nephrology on demand looks like they are another group making good progress in this mission. Look out UpToDate, Web 2.0 has you in our sights.
- Posted using BlogPress from my iPad
