@weddellite @kidney_boy surprising how many times this comes up in conversation http://t.co/wUkwhetjqg
— Ron Mills (@O2ron) June 26, 2014
Thursday, June 26, 2014
Nephrology oscars
The Greatest Movie Scene (intravenous fluids division) goes to...Catch 22
Tuesday, June 24, 2014
Wednesday, June 18, 2014
Lowest potassium I have seen
The Story
A young woman loses consciousness at home and is unable to be revived. EMS brings her to the hospital with resuscitation in progress.Initial ECG:

Initial labs:
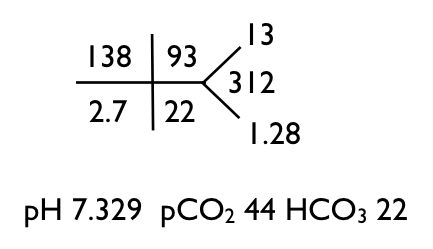
What's the acid base disorder?
I look at the increased pCO2 and decreased pH and call it a respiratory acidosis. The HCO3 should go up to compensate for the increased CO2 but it is slightly decreased, so there is also a metabolic acidosis.
When there is a metabolic acidosis check the anion gap (and even when there is no evidence for a metabolic acidosis, you should check for an anion gap). Holy Ketones, the anion gap is 23!
A large anion gap in the face of only a modest drop in bicarb is unexpected. One expects the bicarbonate to fall 1 mEq/L for every 1 mEq/L the anion gap rises. So if this lady started with an anion gap of 12, her gap went up by 11, so the bicarb should have fallen by 11. In order for the bicarbonate to fall by 11 and end up at 22 it would need to start at 33, indicating a preexisting metabolic alkalosis (or compensated respiratory acidosis I suppose). The metabolic alkalosis is welcome because it fits with the hypokalemia rather well. Alaklosis and hypokalemia go together like macaroni and cheese.
So what is causing the increased anion gap? Well that is easy to determine in this case, her lactate was 12.4, almost a perfect match for an increase in the anion gap of 11. Remember the anion gap is quantifying an anion that is not in the chem-7 but is making its presence known by the unbalanced number of cations and anions. We expect the unbalance to be between 6 and 12, this is a normal anion gap. Her anion gap is 23, 11 over the limit. This means we need to find the anion that explains this gap of 11. A lactate level of 12.4 neatly explains the increased gap. If you are concerned about the difference between 11 and 12, remember that the calculation of 11 comes from assuming that prior to building up the lactic acid, her anion gap was 12, but it could have been 8 or 10 or 4.
What happens next will shock you (now I'm a real internet writer)
The potassium went down. It went way down...to 1.8, and that, my internet friends, is the lowest potassium I have ever seen. And it is the presumed cause of the cardiac arrest. The ECG normalized with correction of the potassium.


Keep in mind that the entire extracellular compartment normally contains only 56 mmol of potassium. The entire plasma compartment normally contains only 12 mmol of potassium. Also keep in mind that after 810 mmol of potassium she was still hypokalemic.
So what happened after 38 hours?

We overshot, in fact we made her hyperkalemic and needed to start dialysis. The dialysis was inevitable, she remained anuric for days after we started the CRRT, and she was also becoming volume overloaded.
The cause of the hypokalemia is unclear. The one point that I am certain of, though, is this must be a chronic process. She had a documented potassium deficiency of 31 grams of potassium! No acute event could have caused her to lose that much potassium, the process that caused the hypokalemia and metabolic alkalosis must have been going on for weeks? Months? Years? Prior to her developing the cardiac arrhythmia. She has recovered her renal function and her electrolytes remain within normal limits, she does not seem to have any renal leak of potassium that I can detect. She denies vomiting. She does have a poorly documented incident of hypokalemia that happened years ago. Her magnesium when measured on the first hospital day was normal. Since recovering her kidney function her magnesium has been low normal. She denies salt-cravings. Just after she recovered her kidney function and her creatinine was normal, she developed slight hypokalemia, right around 3.2 mmol/L. I shot off a TTKG and it was an unremarkable 3.1.
So smart people on the internet, what do you think caused the hypokalemia. The family is understandably concerned that this could happen again. I have my theory, but I don't want to bias your thoughts. Please e-mail me or DM me on Twitter.
Saturday, June 14, 2014
Monday, June 9, 2014
Hyponatremia Guidelines, coming to #NephJC Tuesday June 10th
Things have been a little slow at PBFluids as I have been putting my energy into NephJC the Nephrology Twitter Journal Club.
NephJC will do it's fourth article next Tuesday and it is an article that breaks the mold. Clinical practice guidelines, like review articles and editorials are usually not included in the cannon of journal club. However we want NephJC to expand these horizons in order to tackle any document that may influence nephrology. Clinical practice guidelines probably have more influence over medicine than any single article and because of that they deserve the same critical eye that research articles do.
The Subject of this week's NephJC is: Clinical practice guideline on diagnosis and treatment of hyponatraemia. It was published in NDT, The European Journal of Endocrinology and Intensive Care Medicine.




There is a little blurb about pseudohyponatremia, despite telling us that this guideline will only cover hypo-osmotic hyponatremia. They point out that despite common opinion that this lab abnormality is no longer a problem that it still continues today:
They have a tidy review of the criteria for SIADH:
 Interesting discussion on the rarity of hypothyroidism as a cause of hyponatremia. I was taught this as a fellow but had never seen any literature to support this pearl:
Interesting discussion on the rarity of hypothyroidism as a cause of hyponatremia. I was taught this as a fellow but had never seen any literature to support this pearl:
I love this figure explaining how the two stimuli for ADH release, volume status and hyperosmolality, interact:

This is great writing on a subject that can be difficult to express:
 If they get better:
If they get better:

















NephJC will do it's fourth article next Tuesday and it is an article that breaks the mold. Clinical practice guidelines, like review articles and editorials are usually not included in the cannon of journal club. However we want NephJC to expand these horizons in order to tackle any document that may influence nephrology. Clinical practice guidelines probably have more influence over medicine than any single article and because of that they deserve the same critical eye that research articles do.
The Subject of this week's NephJC is: Clinical practice guideline on diagnosis and treatment of hyponatraemia. It was published in NDT, The European Journal of Endocrinology and Intensive Care Medicine.
The guideline weighs in at 47 pages but the core guideline is actually only a very meaty 30 pages. It is clearly written by committee with a beautiful contradiction on the third page:
So this CPG is either a definition of the standard of care or its not, who knows.
The scope is hypo-osmolar hyponatremia in adults. The authors start out and focus on the elephant in the room, hyponatremia is defined by an abnormal lab test but the vast majority of patients are not symptomatic and it is unclear how important correcting the sodium is. They created a hierarchy of outcomes which seems well thought out.
The cut-off date for the guidelines was December 2012. They searched the usual subjects for articles. Then they threw in this little nugget, sounds like a sure fire method to generate bias:
We excluded case series that reported on benefit if the number of participants was under 5 but included even individual case reports if they reported an adverse event.
Recommendations were categorized using the GRADE system.
 |
| To interpret the guidelines to come you should major in Grade D, with a minor in Grade C. |
After dispensing with the beurocracy of how the guidelines were written, they start with a review of the physiology of water handling and the etiology of hyponatremia. It is a well written and solid text. A worthy addition to any resident's Evernote.
Hyponatremia occurs in 30% of hospitalized patients. That data comes from Hoorn's exhaustive, but single center, trial at the Erasmus Medical Center in Rotterdam.
According to the American Hospital Association, there are 36 million admissions every year, if we extrapolate Hoorn's data to that number we get 10.8 million U.S. cases of hyponatremia a year and 1 million U.S. cases of profound hyponatremia a year. Keep those numbers in mind as you read the evidence behind the comprehensive guidelines to follow.
The clinical features of hyponatremia.
The authors discuss the commonly expressed symptoms of acute hyponatremia but then spend an entire paragraph focusing on the subtle symptoms of chronic hyponatremia that may easily be missed by history or physical:
Although the more severe signs of acute hyponatraemia are well established, it is now increasingly clear that even patients with chronic hyponatraemia and no apparent symptoms can have subtle clinical abnormalities when analysed in more detail. Such abnormalities include gait disturbances, falls, concentration and cognitive deficits (13). In addition, patients with chronic hyponatraemia more often have osteoporosis and more frequently sustain bone fractures than normonatraemic persons (14, 15, 16). Finally, hyponatraemia is associated with an increased risk of death (17, 18). Whether these are causal associations or merely symptoms of underlying problems such as heart or liver failure remains unclear (19).I wrote an editorial about that last reference for eAJKD.
There is a little blurb about pseudohyponatremia, despite telling us that this guideline will only cover hypo-osmotic hyponatremia. They point out that despite common opinion that this lab abnormality is no longer a problem that it still continues today:
Pseudohyponatraemia was seen more frequently with flame photometric measurement of serum sodium concentration than it is now with ion-selective electrodes, but despite common opinion to the contrary, it still occurs (30), because all venous blood samples are diluted and a constant distribution between water and the solid phase of serum is assumed when the serum sodium concentration is calculated (30)Thought the "it still occurs" loses some punch when one references an 11 year old article.
They have a tidy review of the criteria for SIADH:
Although included in many diagnostic algorithms, hypothyroidism very rarely causes hyponatraemia (49). In 2006, Warner et al. (50) observed that serum sodium concentration decreased by 0.14 mmol/l for every 10 mU/l rise in thyroid-stimulating hormone, indicating that only severe cases of clinically manifest hypothyroidism resulted in clinically important hyponatraemia. Development of hyponatraemia may be related to myxoedema, resulting from a reduction in cardiac output and glomerular filtration rate (51).Then they have a shout out to icodextrin-based PD fluid inducing hyponatremia. This was on my nephrology recertification boards.
I love this figure explaining how the two stimuli for ADH release, volume status and hyperosmolality, interact:
Depending on the kidney’s ability to dilute urine, 50–100 mmol of solutes, such as urea and salts, are required to remove 1 l of fluid. If solute intake is low relative to water intake, the number of available osmoles can be insufficient to remove the amount of water ingested.
Guidelines for the diagnosis of the etiology of hyponatremia
Finally on page 17 of the guideline we get the first guideline: The Classification of hyponatremia, they have three different systems for classifying hyponatremia, none of them based on volume status: |
| Table 5. What? No hiccups? |
- Biochemical severity
- Mild: Na 130-135
- Moderate: 125-130
- Profound: less than 125
- Time-based
- Acute: duration less than 48 hours
- Chronic: duration at least 48 hours
- Symptom based
- moderately symptomatic (based on Table 5)
- Severely symptomatic (based on Table 5)
An explanation for why they went with Mild, Moderate and Profound (rather than severe):
Authors mostly use the terms ‘mild’, ‘moderate’ and ‘severe’ (61, 62, 63). We have chosen to replace ‘severe’ by ‘profound’ to avoid confusion with the classification based on symptoms, for which we have reserved the term ‘severe’.
Note to authors: changing the classic hierarchy of mild moderate and severe with mild moderate and profound does not avoid confusion.
In regards to symptoms, the authors explain that they very specifically excluded a category of asymptomatic:
The authors defend not using volume status to categorize hyponatremia at least partly due to the pathetic job physicians do at assessing volume status:
Another interesting statement was in regards to using the urine osmolality to determine if ADH is present or not, It is clear that ADH is present when the urine osmolality is greater than serum osmolality and it is clear that ADH is absent when urine osmolality is less than 100 mOsm/Kg, but they identify a grey area from a urine osmolality of 100 to a urine osmolality that isotonic where they say one is unable to definitely say there is ADH or not. (refs: Nephron Physiology and Journal of Emergency Medicine) I found myself in that no man's land in this case.
Urine sodium was examined as a test to separate volume depleted hypovolemia from SIADH. Urine sodium less than 30 was highly sensitive for hypovolemia (0.87-1.0) even in the one series that looked at patients on diuretics separately. However urine sodium has disappointing specificity (i.e. low urine sodium in a patient with SIADH) (0.24 to 0.83).
The authors gave cautious enthusiasm for the fractional excretion of urea less than 12% indicating SIADH. One case series had the FEUrea with a sensitivity of 0.86 and specificity of 1.0.
It is interesting though, that when they made their flow chart, the lack of precision of urine sodium, urine osmolality, physician ability to discriminate volume status are all thrown out the window. Flow charts are loved by students but never allow for the subtle Bayesian realities of clinical medicine.

They use a flow chart to map out when to use the various treatment recommendations. This seems like an intelligent to build what is essentially a table of contents for using the guidelines. Nice job.In regards to symptoms, the authors explain that they very specifically excluded a category of asymptomatic:
We have purposefully omitted the category ‘asymptomatic’ as we believed this might create confusion. Patients are probably never truly ‘asymptomatic’ in the strictest sense of the word. Very limited and subclinical signs such as mild concentration deficits are seen even with mild hyponatraemia (13).They use the Hillier correction factor for hyperglycemia (add 2.4 mmol/L per 100 mg/dl of glucose). I think that is wrong.
The authors defend not using volume status to categorize hyponatremia at least partly due to the pathetic job physicians do at assessing volume status:
We found two studies indicating that in patients with hyponatraemia, clinical assessment of volume status has both low sensitivity (0.5–0.8) and specificity (0.3–0.5) (89, 103). Similarly, it seems that clinicians often misclassify hyponatraemia when using algorithms that start with a clinical assessment of volume status (88). Using an algorithm in which urine osmolality and urine sodium concentration are prioritized over assessment of volume status, physicians in training had a better diagnostic performance than senior physicians who did not use the algorithm (104).Hard to believe that nephrologists are no better at determining hypovolemia than a coin toss. Incredible.
Another interesting statement was in regards to using the urine osmolality to determine if ADH is present or not, It is clear that ADH is present when the urine osmolality is greater than serum osmolality and it is clear that ADH is absent when urine osmolality is less than 100 mOsm/Kg, but they identify a grey area from a urine osmolality of 100 to a urine osmolality that isotonic where they say one is unable to definitely say there is ADH or not. (refs: Nephron Physiology and Journal of Emergency Medicine) I found myself in that no man's land in this case.
Urine sodium was examined as a test to separate volume depleted hypovolemia from SIADH. Urine sodium less than 30 was highly sensitive for hypovolemia (0.87-1.0) even in the one series that looked at patients on diuretics separately. However urine sodium has disappointing specificity (i.e. low urine sodium in a patient with SIADH) (0.24 to 0.83).
The authors gave cautious enthusiasm for the fractional excretion of urea less than 12% indicating SIADH. One case series had the FEUrea with a sensitivity of 0.86 and specificity of 1.0.
It is interesting though, that when they made their flow chart, the lack of precision of urine sodium, urine osmolality, physician ability to discriminate volume status are all thrown out the window. Flow charts are loved by students but never allow for the subtle Bayesian realities of clinical medicine.
Treatment Guidelines
Treatment of patients with severe symptoms from hyponatremia:
If they don't get better:
If you can't tell if they got better, assume they did.
This is how I put these recommendations together:
It was interesting to see them review all of the cases of osmotic demyelination, to paraphrase Churchill:
Never has so much been done by so many to avoid a complication that occurs in so few.
Some characteristics of the people who developed osmotic demyelination:
The speed limit for correction of hyponatremia:
Treatment of patients with moderately severe symptoms from hyponatremia:
Remember moderate symptoms include headache, nausea (without vomiting), and confusion. I would be reluctant to use 3% in a lot of patients that look like they fit this recommendation. They even recommend 3% saline in some cases of for acute yet asymptomatic patients. The speed limit, 10 mmol/L the first day and 8 mmol/L per day after that remains the same.
Treatment of patients without severe of moderately severe symptoms from hyponatremia:
What the rest of the world calls asymptomatic hyponatremia.
They sure like their 3%. Here again, even in asymptomatic patients they recommend possibly giving 3%. The most surreal moment in this clinical practice guideline is when they reference a randomized trial of 8 ultra-marathoners in the Western States Endurance Run. Like this has any relevance to my patients in the hospital, where endurance is measured in steps, not miles.
Treatment of patients with chronic hyponatremia without severe or moderately severe symptoms:
They divide their recommendations into general recommendations, and then recommendations for patients with volume expansion, SIADH, and reduced circulating volume.
7.4.1. general management. They recommend against treating the serum sodium if it is above 130. This implies that sodiums below 130 should be corrected for the sake of the number alone.
In 7.4.2 they drill down into patients with expanded extracellular volume. Here they advise against treating sodiums above 125. They also recommend against using vasopressin antagonists.
This seems crazy to me. Vaptans are the best studied drugs in the whole field of hyponatremia. No other therapy for low sodiums has any type of reasonable rigorous clinical trials to support its use. Look at the description of the studies they sight to support the use of hypertonic saline in acute symptomatic hyponatremia:
It's all case series and retrospective crap. Compare that to the thousands of patients who have used vaptans safely to raise their sodiums. The authors reference two reviews, the first with 15 RCTs of vaptans with 1,619 patients and the other with 11 RCTs and 1,094 patients. In neither of these reviews were there any episodes of osmotic demyelination despite increased risk for overly rapid correction of sodium with vaptans. The authors found 5 more trials outside of those reviews bringing the total number of patients examined in RCTs to 2,900. The authors own analysis of the data found a signal indicating a possible increased risk of death in hypervolemic patients. See appendix 6:
 |
| appendix 1-5 then 7 and then 6. Cause that's how European's count. |
So what do they mean by signal indicating a possible increase risk of death? Here is the forrest plot from the appendix:
1.19.4 is the analysis they called out. Three studies, two using oral lixivaptan and one using satavaptan. I guess I was reassured to see that this signal (code for non-signifigant data) does not come from any of the licensed vaptans in the US. One of the reason it feels a bit like a hit job is they could have just as easily pointed out this chart where it looks like there is a survival signal for conivaptan.
Of note: the manufacturer of tolvaptan, has warned that some patients with rapid increases of sodium due to tolvaptan have suffered neurologic sequelae, though the authors could not find any reports in the literature.
The next guidelines are for SIAD where again they recommend against using vaptans, but now add lithium or demeclocycline to the list. They recommend using fluid restriction and if that doesn't work, use urea, or the combination of a loop diuretic and salt tablets. No randomized controlled trials of any of these therapies were found. In addition they reported two cases of osmotic demyelination in patients who had fluid restriction, though it seems unlikely that fluid restriction was the primary culprit.
In their defense of the guidelines they had these wonderful paragraphs:
The last section of the guideline addresses what to do if the sodium goes up too fast.
And that is the last guideline. I look forward to discussing this on Tuesday night at NephJC at 9pm eastern.
Friday, June 6, 2014
Bakris and Agarwal together? It is Nerdtastic
I have heard it argued that no one does more creative clinical hypertension research than Rajiv Agarwal at Indiana University. I am a believer. His latest work is demonstrating the effectiveness of chlorthalidone down into stage 4 CKD, an area previously deemed off limits to thiazide diuretics.
He did a video chat with George Bakris for Medscape discussing the work. Check it out.

I worked with Dr. Agarwal when I was a resident and he was one of those attendings that every resident held in highest regard. Super smart. I was honored when he agreed to write a letter of recommendation for my nephrology fellowship.
Agarwal R, Sinha AD, Pappas MK, Ammous F. Chlorthalidone for poorly controlled hypertension in chronic kidney disease: an interventional pilot study. Am J Nephrol. 2014;39(2):171-82.
He did a video chat with George Bakris for Medscape discussing the work. Check it out.
I worked with Dr. Agarwal when I was a resident and he was one of those attendings that every resident held in highest regard. Super smart. I was honored when he agreed to write a letter of recommendation for my nephrology fellowship.
Agarwal R, Sinha AD, Pappas MK, Ammous F. Chlorthalidone for poorly controlled hypertension in chronic kidney disease: an interventional pilot study. Am J Nephrol. 2014;39(2):171-82.
Wednesday, June 4, 2014
Kidney Stone Teaser
 A patient is a recurrent stone former. The stones are conformed to be calcium oxalate. You put him on UroCitK and he is stone free for 3 years. But he gets lazy and stops taking the drug.
A patient is a recurrent stone former. The stones are conformed to be calcium oxalate. You put him on UroCitK and he is stone free for 3 years. But he gets lazy and stops taking the drug.He then gets started on a drug for migraines which works great. Migraines stop.
Six months later he develops an acute stone. The stone is removed by urology and identified as calcium phosphate. What was the migraine
drug?
Monday, June 2, 2014
PBFluids turns 6 years old
Happy Blog Birthday PBFluids!
 Despite a slow few weeks, I have been focusing on the Twitter Nephrology Journal Club, 2014 has been a solid year for PBFluids.
Despite a slow few weeks, I have been focusing on the Twitter Nephrology Journal Club, 2014 has been a solid year for PBFluids.- This is post number 681
- I have 57 posts in draft, most likely never to see the light of day
- Total page views will squeak over 800,000 by the end of June
The nephrology blogosphere has thinned out a bit in the last year with The Kidney Doctor and Mahesh’s Top Reads going silent. The Kidney Doctor story is a bit strange because it looks like he lost control of his sweet TheKidneyDoc.org URL and had to go with the somewhat less glamorous kidney2.blogspot.com URL.
Another casualty of the last year has been HemoDoc. Where did he go?
LVHN was a new blog run by a fellowship program. It started out with some promising posts but lately has deteriorated into a link blog, with little editorial content.
RedBeans was the other fellowship program blog that started last year and it has continued to produce nice educational content.
I can't think of any new nephrology blogs. A bit disappointing but the social media landscape for nephrology has gotten quite a bit richer despite the loss of blogs. DreamRCT and NephJC were successful new initiatives. NephMadness and Top Nephrology Stories of the Year have matured from early beginnings. And I am excited to announce that we have clawed our way into Kidney Week with the first social media symposium in Philadelphia next November!
Should be an exciting year.
This week's JAMA has a couple of vitamin studies
One positive:
One negative
Pregnant women and people with AIDS seem to be two population where vitamins and supplements have a better track record. Everywhere else is just a wasteland of negative trials.
Vitamin C Supplementation for Pregnant Smoking Women and Pulmonary Function in Their Newborn Infants: A Randomized Clinical Trial (PDF)
One negative
Effect of Vitamin D3 on Asthma Treatment Failures in Adults With Symptomatic Asthma and Lower Vitamin D Levels. The VIDA Randomized Clinical Trial (PDF)
Pregnant women and people with AIDS seem to be two population where vitamins and supplements have a better track record. Everywhere else is just a wasteland of negative trials.
Subscribe to:
Posts (Atom)
