Aldosterone is a bad actor. It is cardiotoxic. It drives a lot of hypertension. It is likely a progression factor in chronic kidney disease. (presentation with a lot of references to the primary data by Adrian Covic can be found here).
This is why aldosterone antagonists are such effective drugs in heart failure, such good antihypertensive agents and have potential in CKD. ACEi and ARB lower aldosterone because one of the two primary stimulants for aldosterone release is angiotensin 2. But about half of patients started on RAAS inhibition experience something called aldosterone escape, where within a few weeks of starting drug therapy, aldosterone levels returns to pre-treatment levels. I suspect a lot of this escape is mediated via increases in potassium.
Aldosterone Escape from joel topf on Vimeo.
The addition of patiromer in a situation like this could lower aldosterone levels and result in improved outcomes. So my call for outcome studies beyond changes in serum potassium is not a plot to derail the drug but to give the drug an opportunity to prove how it can actually improve renal and CV outcomes independent of just allowing patients to stay on RAAS inhibition.
The key is that if the studies are not done we will not know.
Saturday, January 30, 2016
Patiromer and patient oriented outcomes
Recently I have been tweeting back and forth with some biotech investors that have some strong feelings about patiromer. The recuring pro-patiromer theme is the drug will allow people to stay on their ACE inhibitor or angiotensin receptor blocker without fear of hyperkalemia. This is not a stretch belief by team patiromer, it was one of the figures in the supplementary material of the NEJM study:
 So if what we say about ACEi and ARBs is true, staying on them is a good thing. But do we need to do a clinical trial to determine if the benefits of RAAS inhibition are also seen in patients who can only tolerate RAAS inhibition with the addition of a potassium binder? I think we do. Here is my logic.
So if what we say about ACEi and ARBs is true, staying on them is a good thing. But do we need to do a clinical trial to determine if the benefits of RAAS inhibition are also seen in patients who can only tolerate RAAS inhibition with the addition of a potassium binder? I think we do. Here is my logic.
The benefits of RAAS inhibition in CKD are not dramatic:
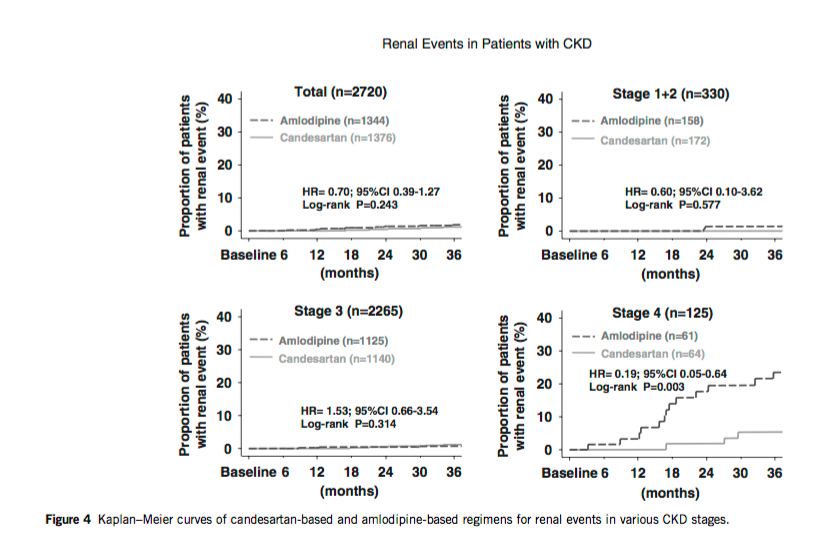
In patients with microalbuminuria, it is difficult to find any clean win. The PREVEND trial and the CASE-J trial (PDF) both showed a benefit in sub group analysis (stage 4 patients, but not in any other stages):
The TRANSCEND trial did not show a renal benefit from the ARB, telmasartan, but in post hoc analysis, patients with albuminuria did have fewer renal outcomes. But subgroup analysis of negative studies is generally considered poor form. Do you really believe that telmasartan increases renal outcomes in the absence of proteinuria, another post-hoc finding.
In the end the recommendation for ACEi and ARB with microalbuminuria in KDIGO gets only a 2D recommendation:
 The NNT to prevent the composite end-point of ESRD or doubling of serum creatinine is a robust 14!
The NNT to prevent the composite end-point of ESRD or doubling of serum creatinine is a robust 14!
Of note from this study 4% of patients were withdrawn due to ACEi side effects, which included the dreaded hyperkalemia.

But the question that I have; the question that nags at me, is, "Are the patients that live at the left end of the bell curve, the ones that were unable to tolerate the ACEi due to hyperkalemia, do they have the same physiology and neurohormonal milieu as the rest of the cohort? Could those patients have naturally low angiotensin 2 levels or low aldosterone levels?" It seems likely.

And if that is the case, it also seems more likely that these patients would be among the 13 patients in our NNT of 14 that do not benefit by not doubling their creatinine or going on dialysis. It's like their bodies have endogenous RAAS inhibition.

If that is the case, that these patients do not benefit from RAAS inhibition then they are not harmed by stopping the drug and hence they would not get a benefit from patiromer.
The essential issue is that though we have shown a benefit of RAAS inhibition for renal outcomes in CKD, we have never shown that benefit in patients who could not tolerate the drug and I think the sliver of patients who cannot tolerate RAAS inhibition may represent a population different enough from the whole cohort to deserve study.
I plan on using patiromer in my patients but it is hard to be a cheer leader for the drug or feel that it is an essential part of the treatment regiment until we see the benefit in this targeted population.

And got this hit:

My search criteria was almost a perfect match for the title of the article. The article shows worse outcomes for patients with increased serum potassium but it did not separate out people by the change in serum potassium or look at renal potassium handling, both of which would be ideal. But that said, there is no signal that increased potassium is a harbinger of increased benefit from ARBs.
Take a look at the response too.

The benefits of RAAS inhibition in CKD are not dramatic:
In patients with microalbuminuria, it is difficult to find any clean win. The PREVEND trial and the CASE-J trial (PDF) both showed a benefit in sub group analysis (stage 4 patients, but not in any other stages):
 |
| Renal outcomes by CKD stage (doubling of sCr, Cr>4, dialysis) |
 |
| No benefit in the whole cohort |
 |
| Anyway you cut it renal function deteriorated faster with ARB |
"The Work Group suggests ACE-Is or ARBs as the preferred class of BP-modifying agent in CKD patients with microalbuminuria. This recommendation is based on observational data and subgroup and post hoc analyses, hence the grade of 2D."On the other hand the data on macroproteinuria, even in non diabetics is not subtle:
These trials include RCTs in patients with CKD of various causes, primarily glomerulonephritis,191 African-Americans with hypertension, and patients with advanced CKD (a GFR of 20–70ml/min/1.73m2). A meta-analysis of in- dividual patient data from 11 RCTs compared antihypertensive regimens including ACE-Is to regimens without ACE-Is in 1860 patients with predominantly non-diabetic CKD. In adjusted analyses, ACE-Is were associated with a HR of 0.69 for kidney failure (95% CI 0.51–0.94) and 0.70 for the combined outcome of doubling of the baseline SCr concentration or kidney failure (95% CI 0.55–0.88). Patients with greater urinary protein excretion at baseline benefited more from ACE-I therapy (P 1⁄4 0.03 for kidney failure and P 1⁄4 0.001 for the combined outcome).Here are some of the key figures from the above mentioned meta-analysis (11 studies, 1,860 non-diabetic patients, RCT ACE-i vs non-ACEi) from Annals of Internal medicine:
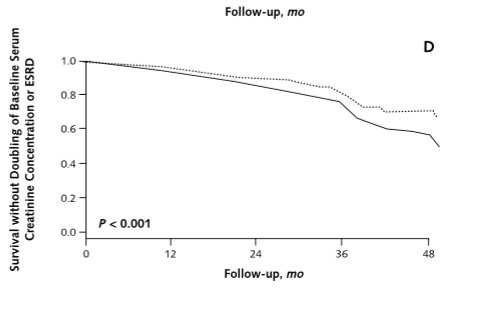 |
| Those lines are diverging over time. Right? |
 |
| Looks like a solid RR of 0.6 to 0.7 with ACEi |
 |
| The higher the proteinuria the greater the benefit. |
 The NNT to prevent the composite end-point of ESRD or doubling of serum creatinine is a robust 14!
The NNT to prevent the composite end-point of ESRD or doubling of serum creatinine is a robust 14!Of note from this study 4% of patients were withdrawn due to ACEi side effects, which included the dreaded hyperkalemia.
But the question that I have; the question that nags at me, is, "Are the patients that live at the left end of the bell curve, the ones that were unable to tolerate the ACEi due to hyperkalemia, do they have the same physiology and neurohormonal milieu as the rest of the cohort? Could those patients have naturally low angiotensin 2 levels or low aldosterone levels?" It seems likely.

And if that is the case, it also seems more likely that these patients would be among the 13 patients in our NNT of 14 that do not benefit by not doubling their creatinine or going on dialysis. It's like their bodies have endogenous RAAS inhibition.

If that is the case, that these patients do not benefit from RAAS inhibition then they are not harmed by stopping the drug and hence they would not get a benefit from patiromer.
The essential issue is that though we have shown a benefit of RAAS inhibition for renal outcomes in CKD, we have never shown that benefit in patients who could not tolerate the drug and I think the sliver of patients who cannot tolerate RAAS inhibition may represent a population different enough from the whole cohort to deserve study.
I plan on using patiromer in my patients but it is hard to be a cheer leader for the drug or feel that it is an essential part of the treatment regiment until we see the benefit in this targeted population.
--UPDATE--
So I received this tweet from David Goldfarb
@kidney_boy what about possibility that hyperK on RAASi means that RAAS is MORE activated? that rise in K is assay for effective drug?
— David S Goldfarb (@weddellite) February 1, 2016
I replied:
@weddellite has anybody done TTKG before and after ACEi and correlated it with clinical outcomes? Does ↓ TTKG ☞ improved outcomes?
— Joel Topf (@kidney_boy) February 1, 2016
Then I entered the following search:

My search criteria was almost a perfect match for the title of the article. The article shows worse outcomes for patients with increased serum potassium but it did not separate out people by the change in serum potassium or look at renal potassium handling, both of which would be ideal. But that said, there is no signal that increased potassium is a harbinger of increased benefit from ARBs.
Take a look at the response too.
Thursday, January 21, 2016

{kind=link}
{kind=link}
Tuesday, January 19, 2016
How much work is the social media internship thingy anyways?
The deadline to apply for the nephrology social media internship is approaching. You have just until this Sunday to get your application in. We have been getting some questions about how much work there is and who the program is designed for.
I'm a critical care doctor. Can I join the internship?
I'm a nurse. Can I join the internship?
I'm a medical student. Can I join the internship?
I'm an attending nephrologist. Can I join the internship?
I don't like nephrology. Can I join the internship?
We designed the program for people in the nephrology space. The mentors in the program are all nephrologists and have all focused on developing social media for doctor to doctor communication channels. However, we feel the lessons are broadly applicable to many communication channels. If you want to develop skills for patient to patient communication or doctor to patient social media the the experience you gain in the internship will be helpful. That said, the assignments and the hands-on experiences will be in nephrology and will be doctor to doctor in nature.
We encourage nurses, doctors in other specialties, and physicians all through the education spectrum from med student to professor emeritus to apply because we will be able to provide you novel tools for interacting in the digital world. We also would love to learn from your carried backgrounds.
I'm a resident. What type of time commitment can I expect?
I'm a med student. What type of time commitment can I expect?
I'm a new mom. What type of time commitment can I expect?
I'm a new mom of twins. What type of time commitment can I expect?
I'm a surgery intern and a new mom of twins. What type of time commitment can I expect?
As a member of the NSMC internship we expect you to participate in as many #NephJCs as possible. This represents 2 hours a month of chat time and probably 2 more hours prepping or doing work surrounding the chats. We may ask you to prepare a summary of an article or curate a Storify after a chat. So call that 4 hours a month, though most months should be less than that.
Then we have two tent pole features a year that you will be required to participate in. These are NephMadness and DreamRCT. These are longer term projects that will likely take between 3 and 6 hours depending on personal commitment and efficiency.
Lastly we encourage the interns to maintain a social media presence. This could be blogging or participating in twitter. This could mean lurking or talking. Many of the people interested in the program already do that. If you do not, however we would ask you to devote some time to being present in our virtual community.
Lastly we will do 3 or 4 Google Hangouts to discuss how the program is going and upcoming plans.
In summary we are looking for an hour a week for the NephJC, two larger assignments that will take a dedicated evening or two, quarterly conference calls or video chats and some time on social media.
If you are interested or have questions, feel free to send us an e-mail. If you want to apply for a spot drop us an e-mail and explain:
The due date for the application is January 24. We will make our decisions and start the program on February 1.
I'm a critical care doctor. Can I join the internship?
I'm a nurse. Can I join the internship?
I'm a medical student. Can I join the internship?
I'm an attending nephrologist. Can I join the internship?
I don't like nephrology. Can I join the internship?
We designed the program for people in the nephrology space. The mentors in the program are all nephrologists and have all focused on developing social media for doctor to doctor communication channels. However, we feel the lessons are broadly applicable to many communication channels. If you want to develop skills for patient to patient communication or doctor to patient social media the the experience you gain in the internship will be helpful. That said, the assignments and the hands-on experiences will be in nephrology and will be doctor to doctor in nature.
We encourage nurses, doctors in other specialties, and physicians all through the education spectrum from med student to professor emeritus to apply because we will be able to provide you novel tools for interacting in the digital world. We also would love to learn from your carried backgrounds.
I'm a resident. What type of time commitment can I expect?
I'm a med student. What type of time commitment can I expect?
I'm a new mom. What type of time commitment can I expect?
I'm a new mom of twins. What type of time commitment can I expect?
I'm a surgery intern and a new mom of twins. What type of time commitment can I expect?
As a member of the NSMC internship we expect you to participate in as many #NephJCs as possible. This represents 2 hours a month of chat time and probably 2 more hours prepping or doing work surrounding the chats. We may ask you to prepare a summary of an article or curate a Storify after a chat. So call that 4 hours a month, though most months should be less than that.
Then we have two tent pole features a year that you will be required to participate in. These are NephMadness and DreamRCT. These are longer term projects that will likely take between 3 and 6 hours depending on personal commitment and efficiency.
Lastly we encourage the interns to maintain a social media presence. This could be blogging or participating in twitter. This could mean lurking or talking. Many of the people interested in the program already do that. If you do not, however we would ask you to devote some time to being present in our virtual community.
Lastly we will do 3 or 4 Google Hangouts to discuss how the program is going and upcoming plans.
In summary we are looking for an hour a week for the NephJC, two larger assignments that will take a dedicated evening or two, quarterly conference calls or video chats and some time on social media.
If you are interested or have questions, feel free to send us an e-mail. If you want to apply for a spot drop us an e-mail and explain:
- Who you are
- Why you want to do the social media internship
- What experience do you already have with social media (Do not be embarrassed to say none. Do not be embarrassed to say you are really good at Facebook quizzes, we respect that)
The due date for the application is January 24. We will make our decisions and start the program on February 1.
The email address is: NephrologyJC@gmail.com
Monday, January 11, 2016
Why is the FENa elevated in acute tubular injury?
Tonight there is a twitter chat on this article

The chat is at 9:00 PM EST, with hashtag: #JHMChat.
The paper is a good review of the weaknesses of both the fractional excretion of sodium and urea. I have a few critiques of the article but one in particular is too complex to express in a tweet, so time to fire up PBFluids once again.
Before we move on, a quick reminder of exactly what FENa measures:
In the paper they describe why patients with AKI get an increased fractional excretion of sodium:
The problem with this model should be quickly obvious, intrinsic renal failure is not a sodium wasting state, in fact these patients have the opposite problem of sodium retention, fluid overload and hypertension. So we have a calculation that shows increased sodium wasting but we have a clinical scenario which shows sodium retention.

The chat is at 9:00 PM EST, with hashtag: #JHMChat.
The paper is a good review of the weaknesses of both the fractional excretion of sodium and urea. I have a few critiques of the article but one in particular is too complex to express in a tweet, so time to fire up PBFluids once again.
Before we move on, a quick reminder of exactly what FENa measures:
 |
| Reminder of what the FENa measures, excreted sodium divided by filtered sodium |
In the paper they describe why patients with AKI get an increased fractional excretion of sodium:
In normal health, FeNa is typically 1%, although it may vary depending on the dietary sodium intake. The corollary is that 99% of filtered sodium is reabsorbed. Acute tubular injury (ATI) that impairs the tubular resorptive capacity for sodium may increase FeNa to >3%.This view of the increased FENa of intrinsic renal failure envisions a world where the kidney needs to reabsorb approximately 99% of filtered sodium to remain in sodium balance, then when the tubules are damaged by acute tubular injury they fail in that job and begin to waste sodium.
 |
| The view of FENa as expressed in the article by Pahwa and Sperati |
The problem with this model should be quickly obvious, intrinsic renal failure is not a sodium wasting state, in fact these patients have the opposite problem of sodium retention, fluid overload and hypertension. So we have a calculation that shows increased sodium wasting but we have a clinical scenario which shows sodium retention.
The way out of this paradox is that damaged nephrons do not waste sodium. When the tubule suffers acute tubular injury, filtered sodium (and chloride) fails to be reabsorbed in the proximal tubule and thick ascending limb of the loop of Henle. This flood of unreabsorbed chloride trips sensors in the juxtaglomerular apparatus and shuts down the glomeruli. This is the nature of tubular glomerular feedback (TG feedback).
It is also (at least) part of the reason the histologically intact glomeruli have a GFR of zero. The damaged tubule sends an SOS to the glomeruli telling it to shut down. If the tubules cannot reabsorb sodium it is essential that the glomeruli stop filtering. A kidney that filters but fails to reabsorb will pee the patient to death in a matter of minutes (GFR of 100 mL per minute will excrete all of the plasma volume in 30 minutes) The kidney (teleologically speaking) is programmed to never let this urinary nightmare happen.
So if in acute tubular injury, the damaged tubules do not provide the urine used to assess FENa, where does that urine come from? It comes from the intact nephrons. Remember acute tubular injury is a patchy diagnosis, with some regions of the kidney being affected and others being relatively spared. It is the unaffected nephrons that produce the urine in acute tubular injury that has the high fractional excretion of sodium. Why is that? It is best to look at what happens to FENa in normal patients as CKD progresses.
In a patient with a GFR of 100 ml/min and a sodium intake consistent with current guidelines, 100 mmol/day (2.3 grams sodium), the average fractional excretion of sodium will be:
 |
| TG Feedback in action. A failure to reabsorb Na (and Cl) means that excess distal delivery of chloride will trip the JGA and shut down the glomeruli. |
It is also (at least) part of the reason the histologically intact glomeruli have a GFR of zero. The damaged tubule sends an SOS to the glomeruli telling it to shut down. If the tubules cannot reabsorb sodium it is essential that the glomeruli stop filtering. A kidney that filters but fails to reabsorb will pee the patient to death in a matter of minutes (GFR of 100 mL per minute will excrete all of the plasma volume in 30 minutes) The kidney (teleologically speaking) is programmed to never let this urinary nightmare happen.
So if in acute tubular injury, the damaged tubules do not provide the urine used to assess FENa, where does that urine come from? It comes from the intact nephrons. Remember acute tubular injury is a patchy diagnosis, with some regions of the kidney being affected and others being relatively spared. It is the unaffected nephrons that produce the urine in acute tubular injury that has the high fractional excretion of sodium. Why is that? It is best to look at what happens to FENa in normal patients as CKD progresses.
In a patient with a GFR of 100 ml/min and a sodium intake consistent with current guidelines, 100 mmol/day (2.3 grams sodium), the average fractional excretion of sodium will be:
- Excreted sodium = daily sodium intake = 100 mmol/day
- Filtered sodium = 0.1 L/min x 140 mmol/L x 1,440 min/day = 20,160 mmol/day
- FENa (excreted Na/ filtereed Na) = 0.5%
Notice how in this situation if we increase the sodium intake to better correlate with the typical American diet of 200 mmol/day of sodium per day the FENa increases to 1% without changing the volume status one bit. With stable renal function, FENa is a measure of sodium intake not volume status.
If this same patient now has a GFR of 20 mL/min and the same 100 mmol of sodium intake, the data looks like this:
- Excreted sodium = daily sodium intake = 100 mmol/day
- Filtered sodium = 0.02 L/min x 140 mmol/L x 1,440 min/day = 4,032 mmol/day
- FENa (excreted Na/ filtereed Na) = 2.4%
This situation is not an acute disease state. The patient has CKD, but stable renal function. They do not have acute tubular injury. They just have a decreased, but stable, GFR. The increase in FENa means that to get rid of the same sodium load, more of the filtered sodium needs to be excreted. This is what is happening in the undamaged tubules of intrinsic renal failure. The damaged tubules are shut down due to TG feedback. The undamaged tubules are dealing with the excess sodium load by reabsorbing less sodium, pushing up the FENa.
The FENa is not showing pathologically abnormal tubule response in the damaged tubules but actually showing a physiologically sound response to a decreased GFR from the intact tubules.
So who cares? Why does this matter?
It matters because this understanding allows one to understand why the FENa fails in certain circumstances. To me the three most important places the FENa fails are:
- Acute tubular injury in a patient with burns
- Acute tubular injury in a patient with CHF
- Acute tubular injury in hepatorenal syndrome
In all three of these scenarios the patient will have a low FENa despite the acute tubular injury. The background clinical situation is one where the patient would naturally be very sodium avid. The ATI-damaged tubules are shut down and do not contribute to the urine. The intact tubules however are retaining sodium due to the volume depletion (burns), the heart failure, or the altered physiology of cirrhosis. The low FENa in these scenarios represents the overall sodium milieu and does not rise with the decreased GFR of from the acute tubular injury.
FENa: it's harder than you might think.
I have been called out for not including a reference to the classic article that I base al of my knowledge of AKI on, Acute Tubular Success. My bad. If you like reading stuff like this, dont miss this classic.
@ChristosArgyrop Everything I know about nephrology came from that article. The rest is just commentary.
https://t.co/LPRSBcoGMX
— Joel Topf (@kidney_boy) January 11, 2016
Though @kidney_boy misses citing one of the best paper title (paper on TGF) https://t.co/bOl5TwsvAg #JHMChat pic.twitter.com/69uAjwODVo
— Swapnil Hiremath, MD (@hswapnil) January 11, 2016
Thursday, January 7, 2016
We don't know shit about IV Fluids
I teach IV fluids to every third year medical student and resident that crosses the threshold at St John Hospital. It's what I do. It's a conventional lecture focusing on the expected fluid distribution following various flavors of IV fluids.
The dogma of IV fluids is that dextrose solutions, crystalloids and plasma expanders distribute across the body compartments in unique ways.
Dextrose solutions distribute like total body water, with two thirds disappearing into the intracellular compartment and the remaining third distributing one part to the plasma compartment and three parts to the interstitial compartment. So approximately 80 milliliters of a liter of D5W remains in the plasma compartment.
Isotonic saline is trapped in the extracellular compartment and one quarter of it expands the plasma compartment. So one quarter of a liter of isotonic saline remains in the plasma compartment.
Plasma expanders are locked to the plasma compartment so one liter of albumin expands the plasma compartment by one liter.
So in summary:



The dogma of IV fluids is that dextrose solutions, crystalloids and plasma expanders distribute across the body compartments in unique ways.
Dextrose solutions distribute like total body water, with two thirds disappearing into the intracellular compartment and the remaining third distributing one part to the plasma compartment and three parts to the interstitial compartment. So approximately 80 milliliters of a liter of D5W remains in the plasma compartment.
Isotonic saline is trapped in the extracellular compartment and one quarter of it expands the plasma compartment. So one quarter of a liter of isotonic saline remains in the plasma compartment.
Plasma expanders are locked to the plasma compartment so one liter of albumin expands the plasma compartment by one liter.
 |
| from the label of 4% albumin, the co-star of the SAFE trial |
So in summary:
- one liter of dextrose expands the plasma compartment by 80 mL
- one liter of 0.9% saline expands the plasma compartment by 250 mL
- one liter of 4% albumin expands the plasma compartment by 1,000 mL
These fluids have radically different effects on the plasma compartment so when used for volume resuscitation in critically ill patients we should expect different outcomes. We have empiric data on this. Initially, in the late 90's we were in meta-analysis hell with some saying albumin was poison and others saying there was no difference between the two. Thankfully the Aussies rescued us with a large, well done RCT:

and it showed...nothing:

This blows my mind.
How can a substance that is four times as efficient as another, at least by the metric we think are critical, have no influence on outcome?
Shouldn't radically different efficiencies at expanding the plasma compartment have some signal, either good or bad?
The fact that it made no difference at all makes me think that differentiating them based on their ability to expand the plasma compartment is misguided.
Additionally we didn't even see the 4:1 ratio in efficiency that is expected. Albumin dosing should have been one fourth of saline dosing, but in the study it was only about 70% of saline:

The SAFE trial is impossible for me to integrate into the conventional model of how IV fluids work. Is it time to abandon the model?
Wednesday, January 6, 2016
The second Nephrology Social Media Internship
The first second Nephrology Social Media Internship
 |
| Told you we'd get a logo |
Last year we launched the social media internship with 4 interns. It went well and all of them had a unique and positive experience. They have all graduated from pupil to teacher and are part of the NSMC faculty. The remainder of the faculty remains a star studded cast...I give you the: Nephrology Social Media Collective:

- Swapnil Hiremath, co-founder and brain child of NephJC
- Matt Sparks, savior of Renal Fellow Network and co-creator of NephMadness
- Kenar Jhaveri, blogger at NephronPower and editor of AJKDblog
- Paul Phelan, contributor to NephJC, Renal Fellow Network and AJKDblog
- Jordan Weinstein, creator of UKidney
- Edgar Lerma, creator of #NephPearls hashtag and serial author
- Myself
- Hector Madariaga, former NSMC intern and current transplant fellow at the University of Maryland.
- Scherly Leon, former NSMC intern and second year nephrology fellow SUNY Downstate
- Nikhil Shah former NSMC intern and Home Therapy Fellow at the University of Alberta
- Chi Chu former NSMC intern and second year IM resident in San Francisco
The idea behind the internship is to give guidance to doctors or students who want to become experts in social media. There are a number of different techniques and strategies in social media and we will provide the interns an opportunity to work with these techniques first hand. Projects that the interns will participate in:
- NephMadness
- NephJC
- AJKDblog
- Renal Fellow Network
- Research
- UKidney
- DreamRCT
Technologies that the intern will be exposed to include:
- Podcasts
- Google hangouts
- Tweet chats
- Storify for curation
- Mail Chimp newsletters
- Twitter analytics
- Google analytics
- Simpler analytics
- Multiple blogging engines including:
- Blogger
- WordPress
- Medium
- SquareSpace
But this is not a technology internship. This is a communication internship and we will provide guidance and experience that comes from the faculty's collective wisdom.

Interns get immediate and front row access to a personal learning network of social media masters Jedi.
Each intern really gets to craft an individual experience out of this opportunity and none of their journeys will be the same. This is the first time we are doing the second year of the program and we have learned a lot and have plans to make the experience more fulfilling and rewarding.
I have a fellow, resident and two fourth years. When we do ward rounds there are 5 students. #WhoIsThe5thStudent
— Joel Topf (@kidney_boy) November 17, 2015
We know that you have families, residencies, research and boards to prepare for. We are excited to make social media work for you rather than enslave you. We will be sensitive to your "other life" and all of our projects are relatively time insensitive. For more information outlining the responsibilities and the projected work load see this post.
If you are interested or have questions, feel free to send us an e-mail. If you want to apply for a spot drop us an e-mail and explain:
- Who you are
- Why you want to do the social media internship
- What experience do you already have with social media (Do not be embarrassed to say none. Do not be embarrassed to say you are really good at Facebook quizzes, we respect that)
The email address is: NephrologyJC@gmail.com
Tuesday, January 5, 2016
The wisdom of the Fonz
The Fonz on grading. @joe_bower would be proud. pic.twitter.com/Pg1qv1mvue
— Dean Shareski (@shareski) January 5, 2016
Monday, January 4, 2016
Nephrology Apocalypse
Kenar started it with this tweet and image:
As befits the remix culture we live in Fraz Ahmed Ismat created this derivative:
Kenar concluded it is all about the Benjamins:
Here is my attempt to integrate the money question into the data, I also added a column for career satisfaction. This data is taken from the MedScape 2014 Survey. There was no data on ID or geriatrics so I substituted internal medicine.



Spots and applicants ratio in internal medicine @ASNKidney @Nephro_Sparks @kidney_boy @hswapnil pic.twitter.com/FpsrZd53Zb
— Kenar Jhaveri (@kdjhaveri) January 2, 2016
As befits the remix culture we live in Fraz Ahmed Ismat created this derivative:
@kdjhaveri @ASNKidney @Nephro_Sparks @kidney_boy @hswapnil Fixed your chart. Ranked by unmatched residents. pic.twitter.com/nD69QMNKcO
— Fraz Ahmed Ismat (@fismat) January 3, 2016
Kenar concluded it is all about the Benjamins:
— Kenar Jhaveri (@kdjhaveri) January 4, 2016
Here is my attempt to integrate the money question into the data, I also added a column for career satisfaction. This data is taken from the MedScape 2014 Survey. There was no data on ID or geriatrics so I substituted internal medicine.


The equation for applicant pool compared to positions is (Applicants - Positions) / Positions.
Here is a clearer picture without the bubbles.

Sunday, January 3, 2016
SPLIT trial is coming to NephJC
The SPLIT trial was the long awaited randomized control trial that pitted normal saline against the balanced solution du jour, Plasma Lyte-148. I have never before dedicated to the statistical plan for a study before the wait up to SPLIT:

 I wasn't the only fluids nerd waiting for SPLIT. In the days and weeks after the study dropped at ESCIM in Berlin there was a lot of blog energy expended on the study:
I wasn't the only fluids nerd waiting for SPLIT. In the days and weeks after the study dropped at ESCIM in Berlin there was a lot of blog energy expended on the study:
And let's face it the SPLIT trial did not go the way a lot of us wanted or expected. Everybody that was paying attention to the discussion had joined #TeamBalancedSolution. If you want to get a feel for the sense of inevitability of balanced solutions re-read the description from NephMadness 2014 or check out this editorial in KI.
SPLIT went the other way: it showed no adverse affects from saline and no advantage to balanced solutions. Much of the blogging about SPLT was fairly critical. Much of the criticism focused on the patient population (relatively low risk) and a lot of the criticism focused on the relatively low volume of fluid given to the participants. PulmCrit's discussion on the volume of fluid is typical of much of the criticism:
Shaw, et al. did a beautiful retrospective analysis of 0.9% saline versus Plasma-Lyte with propensity scoring. They showed a litany of problems with 0.9% saline:
How much fluid was needed to provide all of this hazard? About 2 liters of saline and 1.6 liters of Plasma-Lyte:
 One of the bedrock data points that showed harm from saline is Yunos' prospective, but unblinded analysis. Covered here on PBFluids.
One of the bedrock data points that showed harm from saline is Yunos' prospective, but unblinded analysis. Covered here on PBFluids.
Yunos's found the use of saline compared to Hartman's (Australian for Ringer's lactate):
Another highly referenced article in the saline versus balanced solution cannon is Chowdhury's randomized controled trial of healthy volunteers that used MRI imaging to measure renal blood flow following saline compared to plasmalyte 142 infusions. They found a significant reduction in mean renal artery flow velocity (P = 0.045) and renal cortical tissue perfusion (P = 0.008) from baseline with saline, but not Plasma-Lyte 148.

The volume of fluid needed to demonstrate decreased perfusion? Two liters.
After reading and digesting SPLIT, I'm still on #TeamBalancedSolution but my certainty has been shaken because to my mind SPLIT is the best done study with real patient oriented outcomes and it was convincingly negative.
I look forward to a spirited discussion in #NephJC on January 12th at 9pm EST and January 13th at 8 pm GMT.

 I wasn't the only fluids nerd waiting for SPLIT. In the days and weeks after the study dropped at ESCIM in Berlin there was a lot of blog energy expended on the study:
I wasn't the only fluids nerd waiting for SPLIT. In the days and weeks after the study dropped at ESCIM in Berlin there was a lot of blog energy expended on the study:And let's face it the SPLIT trial did not go the way a lot of us wanted or expected. Everybody that was paying attention to the discussion had joined #TeamBalancedSolution. If you want to get a feel for the sense of inevitability of balanced solutions re-read the description from NephMadness 2014 or check out this editorial in KI.
SPLIT went the other way: it showed no adverse affects from saline and no advantage to balanced solutions. Much of the blogging about SPLT was fairly critical. Much of the criticism focused on the patient population (relatively low risk) and a lot of the criticism focused on the relatively low volume of fluid given to the participants. PulmCrit's discussion on the volume of fluid is typical of much of the criticism:
How does this data apply to other situations? A broader interpretation of the study is that administration of 1-2 liters of normal saline would not increase the risk of renal failure compared to plasmalyte. This is not particularly controversial. Even the most ardent supporters of balanced crystalloid would probably agree that fluid selection doesn’t make a big difference at a volume of 1-2 liters. The proposed mechanism of nephrotoxicity due to saline is induction of a hyperchloremic metabolic acidosis, which tends to occur with larger volumes of fluid.
So how does the "low" volume compare to other trials that showed harm from 0.9% NS?
Shaw, et al. did a beautiful retrospective analysis of 0.9% saline versus Plasma-Lyte with propensity scoring. They showed a litany of problems with 0.9% saline:
- In-hospital mortality was 5.6% in the saline group and 2.9% in the balanced group (P < 0.001)
- One or more major complications occurred in 33.7% of the saline group and 23% of the balanced group (P < 0.001)
- Balanced fluid was associated with fewer:
- complications (odds ratio 0.79; 95% confidence interval 0.66-0.97).
- Postoperative infections (P = 0.006)
- Renal failure requiring dialysis (P < 0.001)
- Blood transfusion (P < 0.001)
- Electrolyte disturbance (P = 0.046)
- Acidosis investigation (P < 0.001)
- Acidosis intervention (P = 0.02)
How much fluid was needed to provide all of this hazard? About 2 liters of saline and 1.6 liters of Plasma-Lyte:

Yunos's found the use of saline compared to Hartman's (Australian for Ringer's lactate):
- Mean increase in creatinine while in the ICU was 22.6 μmol/L vs 14.8 μmol/L (P = 0.03)
- The incidence of injury and failure class of RIFLE-defined AKI was 14% vs 8.4% (P <.001)
- The use of acute dialysis was 10% vs 6.3% (P = .005).
Another highly referenced article in the saline versus balanced solution cannon is Chowdhury's randomized controled trial of healthy volunteers that used MRI imaging to measure renal blood flow following saline compared to plasmalyte 142 infusions. They found a significant reduction in mean renal artery flow velocity (P = 0.045) and renal cortical tissue perfusion (P = 0.008) from baseline with saline, but not Plasma-Lyte 148.

The volume of fluid needed to demonstrate decreased perfusion? Two liters.
After reading and digesting SPLIT, I'm still on #TeamBalancedSolution but my certainty has been shaken because to my mind SPLIT is the best done study with real patient oriented outcomes and it was convincingly negative.
I look forward to a spirited discussion in #NephJC on January 12th at 9pm EST and January 13th at 8 pm GMT.
Subscribe to:
Posts (Atom)
