Nephrology, more than other specialties is plagued by misplaced concreteness. We get false senses of precision because of the myriad of equations that spit out results to the milliliter. All of those equations from Kt/V, to water deficits, to IVF brain teasers depend on an estimate of total body water.
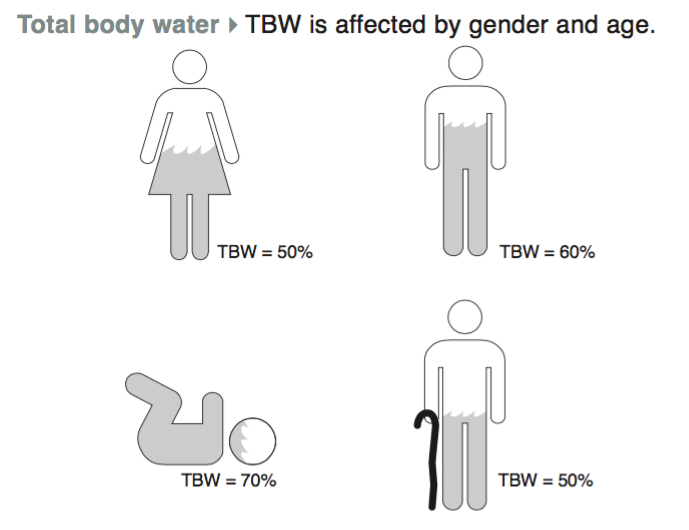
Everyone knows the rule of thumb that young males are 60% water, young females are 50% water and the percent body water falls as people age or get fatter.
Going beyond these rules of thumb, how is total body water measured empirically? The gold standard is heavy water dilution.
This works by giving a sample of heavy water and then waiting for it to equilibrate. Then the investigators measure the heavy water content of exhaled water vapor or a blood sample, the fraction of the water that is heavy water will be equivalent to the fraction of total water which is heavy water. Then since one knows the amount of heavy water given to the patient, one can calculate total body water.
When this is done, or when one reviews the primary literature, as was done in this study the numbers are a little different.
The drop in total body water (in red) in men never gets down to 50% as predicted for the elderly, and in women almost all of the numbers are below 50% and the trend to lower percentages through aging holds if you ignore the 9 women over the age of 70. Of note, these patients are not that obese, see BMIs in blue.
The above study lead to the development of the Watson equation to determine total body water. The Watson equation uses age, weight and height for men and height and weight for women:
Another study of PD patients demonstrated one of my pet peeves, the major effect of obesity has on total body water.
The chart is a bit difficult to understand. The Y axis shows the Watson calculation of total body water minus heavy water dilution. So negative numbers indicates cases where the Watson method underestimates TBW. When the Y-axis is positive the Watson calculation overestimates TBW. The X-axis expresses obesity as body fat over body water. Really? fat over water. You couldn't just graph this versus BMI?
Everyone knows that if you give a liter of saline, all of it remains in the extracellular compartment.
But what if you give a patient just the salt from the saline and none of the water? How much does the solute contribute to the increase in the extracellular volume? How does 154 mmols of NaCl affect the size of the extracellular and intracellular compartments?
Assume the patient is a 70 kg lean young male with a serum osmolality of 280 mOsm/kgH2O. Ignore any renal losses during the process.
For full credit fill out the following:
Total body water:
Size of the extracellular compartment:
Size of the intracellular compartment:
So I checked in at DreamRCT and noticed that my DreamRCT is no longer in the top five.
I'm a big boy and can take this (very minor) form of rejection but I do want to plead my case for a moment. You can read the entire description of my DreamRCT here. One of the dirty little secrets of nephrology is the almost total lack of prospective data on hyponatremia. There are a number of RCTs with regards to tolvaptan, conivaptan and other approved, and soon to be approved, vaptans. But after those there is an evidence desert populated by only a few mirages made up of case reports and retrospective analysis. From this scant data we have built a comprehensive and detailed model of how sodium acts in the body and the importance of osmoregulation. But thats like theoretical physics without a supercollider. We need to test the model with real data.
Think about the fact that hyponatremia is the most common electrolyte disorder. We order metabolic profiles on every patient, every day, but when it comes to interpreting those results we might as well be reading hieroglyphics.
RCTs are difficult and expensive but there are particular areas where we should require them prior to treatment. One of these corners is when we treat people with no symptoms and we are effectively treating a number. High cholesterol, high blood pressure, and low sodiums are three such areas, however hypertension and hypercholesterolemia have both gone through the right of passage called a randomized controlled trial. I am confident that my patients with asymptomatic hypertension benefit from treatment. My patients with coronary disease and hypercholesterolemia will live longer and better with treatment with a high potency statin. On the other hand, patients with sodiums of 129 and no apparent symptoms are supposed to be at higher risk of falls, have a higher mortality from heart and liver failure. Does treating them reduce these risks?
¯\_(ツ)_/¯
We can do better. Hyponatremia is the most common electrolyte disorder found in patients, we owe it to them to have real, prospective, data to answer these questions.
Go to UKidney to vote for my trial: No hyponatremia modification in asymptomatic hyponatremia. Thanks.
DreamRCT is a creative writing project for nephrologists. The assignment is to scour the landscape of nephrology knowledge for a corner that is dominated by dogma and retrospective evidence. Once the target is identified, the writer needs to summarize the gaps, and think up a creative way to shine science's greatest flashlight on the subject, a randomized controlled trial.
We have recruited 16 people to submit DreamRCTs which were published today on MedPage Today. Thanks Ivan, Kristina and Elbert. It is a amazing collection of creativity; there are trials on kidney stones, electrolytes, dialysis, proteinuria and lupus. Please go check them out; read them and see which are great and which should be relegated to The Journal of Craptology.
After reading the DreamRCTs move on over to Jordan Weinstein's excellent UKidney where it is time to channel your inner Mark Cuban and play Shark Tank with the DreamRCTs.
Which trial should be funded which shouldn't. How much should each trial be awarded. You will get $100,000 to distribute among the trials. Think KickStarter meets NIH. You will not be alone in this endeavor. We have recruited an expert panel of clinical researchers to score the trials. At the conclusion of the contest we will look at how the experts spent their cash and how the crowd did. We will also award a small prize to the funder whose distribution best matches the expert panel.
DreamRCT only works if we get a critical mass of people to participate. Please check out the trials at MedPage Today and then go to UKidney to vote with your (completely virtual, don't ask me for a refund) dollars. Announce the project at morning report, assign your fellows to vote and then submit discuss and submit your own DreamRCT, because in the end DreamRCT is not just a game but a shorthand expression for what we need to do to fix nephrology and heal our patients.
This year I worked with Saiyed Muddasser on an article looking at cold dialysate for cardio protection. Take a look at the summary and then go to the eJC site and make a comment.
Apparently there was a weekly quiz and one of the questions was as follows:
And I received an e-mail asking e to answer this question. Lets go through it item by item. The stem sets up a patient with diarrhea induced metabolic acidosis. This is a cause of non-anion gap metabolic acidosis due to GI loss of bicarbonate.
Choice A. This is wrong. The filtered load of bicarbonate is dependent solely on the plasma bicarbonate concentration. The lower bicarbonate concentration seen in all metabolic acidosis would cause decreased not increased filtered load.
Choice B. This is right. Ammonia is produced in the proximal tubule in response to metabolic acidosis and hypokalemia. This is why ammonium excretion is able to be up-regulated due to an acid load. Titratable acid is fixed and can't accommodate an increased acid load. The ammonia production varies depending on metabolic need and chronic diarrhea would up-regualte ammonia production so it could be converted to ammonium in the medullary collecting duct to help clear the excess acid load.
Choice C. This is right. Hydrogen secretion is increased in the distal nephron in response to the metabolic acidosis. This is needed to replace the bicarbonate lost in the stool. Every hydrogen in secreted int eh distal nephron synthesizes a new bicarbonate molecule for the body.
Choice D. This is wrong. Diarrhea causes a non-anion gap or normal anion gap metabolic acidosis.
Choice E. This is right. Hydrogen secretion in the distal nephron is stoichiometrically equivalent to producing new bicarbonate, one cannot happen without the other.
Some of the social media action around this question:
One night that I was on call, I received an interesting patient from the ED.
The patient was confused but walked into the ER and was able to give at least a partial history. They did some initial chemistries and called me with the following results:
This is the kind of lab that grabs your attention.
With that glucose the first thought should be, "Is this DKA?"
Yes.
Beta-hydroxybutyrate: 6 mmol/L
I try to account for the anion gap. So I look at all the anions I measure and see how well they explain the gap. And if I can't account for the majority of the gap I have difficulty sleeping. This patient's gap was 51, 12 is normal which leaves 39 to account for. Only 6 can be accounted for with beta-hydroxybutyrate.
"Is there a lactic acidosis?"
Yes.
Lactate:16
That still leaves 17 mmol/L of unexplained anions.
Propylene glycol is normally due to the solvents used to dissolve IV drips. So usually we see problems in patients who have been in the ICU for awhile.
Propylene glycol is also found in antifreeze and hydraulic fluids.
The molecular weight is 76, so the 8.1 mg/dl represents only about 1 mmol/L, however it may explain the severe lactic acidosis and by stimulating the production of D-lactate it may explain even more of the gap.
Dialysis removes the parent compound and metabolites. Whether patients need to receive fomepizole is less clear. Kraut and Kurtz suggest fomepizole would be beneficial, while others feel less strongly.
Fomepizole not needed in PG toxicity. IMO, propofol, PG, & paracetamol (APAP) should replace phenformin in MUDPILES. https://t.co/B3PTX2cjOc
This question came in after class from a couple of students.
If the urine sodium in volume depletion and the great edematous states (heart failure, liver failure, and nephrotic syndrome) is low how can the urine osmolality be high?
The osmolality of the urine is made up of electrolytes (sodium, potassium and chloride) and non-electrolytes. The non-electrolytes like urea and ammonia will make up the bulk of the osmolality in the small volume of urine that is seen in this clinical setting.
In the advanced electrolyte class (nephrology and critical are fellowship) we look at the electrolyte content of the urine and use it to look at hypo- and hypernatremia more sophistically. For the purpose of medical school, SHELF exams, and USMLE parts 1, 2, 3 you can safely just look at the osmolality of the urine. We are trying to build a model that is understandable and good enough to predict how patients will behave in health and illness. This works pretty good.
The next question also came from a couple of people in class.
In SIADH, you say that the patients are euvolemic, but then you say they retain water via ADH in the medullary collecting duct. How can both of these be true? Won't they become volume overloaded if they retain water.
This is a common question. The key to understanding this takes a bit of a leap of faith. First off, there is no slight-of-hand here. If you do careful water measurements as patients develop SIADH you can measure an increase in total body water. But critically, the increase in water is not progressive and it does not cause clinically significant volume overload. It does not cause pulmonary edema, it does not cause peripheral edema and it does not cause hypertension, all consequences of true volume overload from a positive sodium balance.
One of the reasons that excessive water intake does not cause volume overload is that most of that water (two-thirds) disappears into the intracellular compartment. Just like no one complains of their rings not fitting after drinking a lot of water, having high ADH does not cause interstitial edema.
This image from the lecture needs to be front and center when you think about SIADH: water out of balance, sodium in balance:
The last question for now comes from an e-mail (jtopf@mac.com):
I had a question from the second half of the lecture about treating euvolemic hyponatremia in the case of adrenal insufficiency. I'm having a hard time understanding why urea and salt tablets would help to reverse the hyponatremia. If solute in = solute out and the kidneys are already in sodium balance, how would it increase the solute load in the case of salt tablets? Even if the urine output goes up, won't there still be non-physiological ADH release and concentration of the urine?
So the best way to think about salt and urea tablets is be visualizing this slide from this SIADH lecture:
In SIADH, the secretion of ADH is fixed and maximal. It's like somone is stepping on the gas and can't remove his foot.
Normally the ADH slides from minimal to maximal in order to balance water excretion with variable water intake:
The ADH slider is supposed to indicate that the ADH can slide from minimal activity, resulting in large volumes of urine, to maximal activity, resulting in minimal urine output. As the questioner correctly intuited, the osmolar load is fully excreted. In euvolemic hyponatremia, the slider is jammed to the right. If the urine osmolality (the denominator) is fixed the only way to adjust the urine volume will be to adjust the osmolar load (the numerator). Increasing the osmolar load with a high protein diet or salt tablets or urea pills will raise the numerator and hence increase the urine volume. It's just math. Yes, taking sodium tablets will just result increase the sodium excretion since these patients are in sodium balance, but this additional sodium excretion increases the urine output making it easier for the patient to have less water intake than excretion, the goal for the treatment of hyponatremia.
Here is a link to the resources I used last year. They are largely unchanged. The water and solute lecture is available under the lecture tab. I will continue to edit this post with additional materials and links.
PBFluids has been quiet. Took awhile to just clear the cobwebs to get this post up.
One of the things that has kept me busy has been a project with a company called MedMastery. Franz Wiesbauer was a fan of my fluids book and reached out to me. We worked together to create a curriculum covering body water, diuretics, IV Fluids, sodium and potassium. The full course is about 1,000 slides. But the genius of MedMastery is how they edit and craft the course so it is broken up into an odd fifty 6-minute morsels. It is medical school for Generation Keurig.
MedMastery has opened up a few of the K-cups for promotion.
Art Levinson is the current Chairman of Apple. He was brought on to the board in 2000 during Job's second act and was present for the introduction of the iPod, iTunes and iPhone.
Art Levinson is always introduced as the former CEO of Genentech but I didn't know his story until I read the Herceptin story in Emperor of All Maladies. Turns out Levinson was trained by Nobel Michael Bishop of oncogene fame. In the late 80's Levinson was leading a group pursuing treatment for breast cancer by doggedly tracking a gene called HER-2. Genentech's executives turned away from cancer research after some high profile failures in the 80's. This should have been the end of genentech's role in HER-2 except for the leadership of Levinson. He dodged the bureaucracy, pursued resources and lead a small team to continue work on HER-2. The group produced Herceptin, one of the most important breakthroughs in chemotherapy in the molecular era in, a jaw-dropping, 3 years.
Laureate
Reading that story I can see why Jobs would want him on the Apple board.
As we were gearing up for NephMadness Mealnie Hoenig mentioned that she loved working with the Nephmadness crew because they were "her people." This resonated with me and has become my latest way of looking at the word. This particularly resonated with me when my college roommate introduced me to Public Broadcast Service.
Gene Kranz
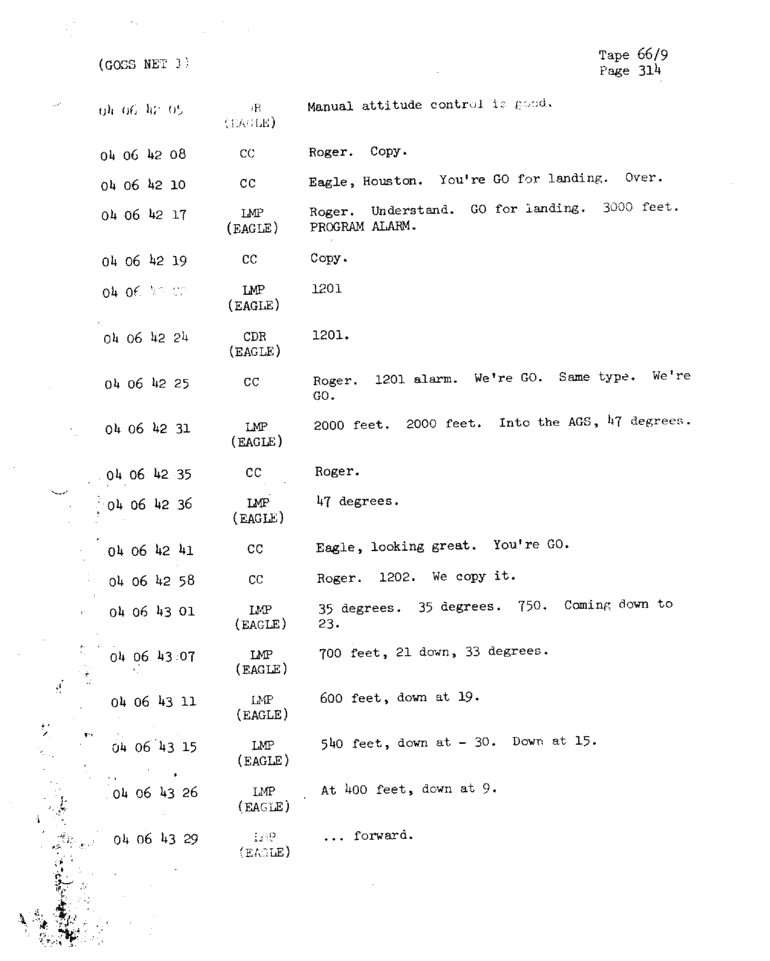
There best song is "Go" which samples Gene Kranz dialog with his flight controllers during the Apollo 11 lunar lander landing. I love this because though I have heard the story of the Apollo mission a 100 times I had never thought of it from the perspective of the flight controllers.
This struck me as a great example of my people. While I never could imagine myself as Neil Armstrong, I could imagine me, and my ilk, being a flight controller in Houston. Which one would I be? flight SURGEON, of course.
Summary of the different flight controllers can be found here.
Transcript from the song:
Narrator (NASA Spokesman?) This is Apollo Control 102 hours into the flight of Apollo 11. It has grown quite quiet here at Mission Control A few moments ago Flight Director Gene Krantz requested that everyone sitdown and get prepared for the events that were coming and he closed with the remark "Good luck to all of you." [Ed. not quite One small step for man; one giant leap for Mankind] 12 minutes now until ignition for powered descent. Everything still looking very good at this point Gene Krantz Okay all flight controllers, "Go" "No go" for powered descent.
CAPCOM we are go for powered descent [CAPCOM, capsule communicator, was an astronaut in Houston responsible for communicating with the mission astronauts. At the time of the landing it was Charlie Duke] We are off to a good start. Play it cool. Okay all flight controllers, I'm going around the horn RETRO? Go! FIDO? Go! GUIDANCE? Go! CONTROL? Go! Deltcom? Go! GNC? Go! EECOM? Go! SURGEON? Go!
Armstrong: Houston...ah...Tranquility base here. The Eagle has Landed.
Kranz: Okay keep the chatter down in this room. [The greatest moment in the history NASA and Kranz is focused on keeping his team on task]
CAPCOM: T1 standby for T1
Kranz: Stay or no Stay all flight controllers [Apparently it was possible to land on the moon but have something go wrong requiring an immediate return to orbit, so this was a check to see if they could proceed to the lunar surface mission]
no need to determine stone composition prior to treating stones
no need to analyze blood chemistry before treating stones
no need to do 24-hour (or 48-hour) urine collections before treating stones
What makes those positions so absurd is that if increased fluid intake did not reduce stones the authors suggested a trial of allopurinol, thiazide diuretics or citrate (without guidance on how to dose, follow or how to choose among those therapies). These recommendations are based on research done on patients where the type of stone had been determined. Not following those enrollment criteria makes the conclusions irrelevant.
It is as if the ACP said not to measure blood pressure because there has never been a randomized controlled trial of patients where blood pressure was measured versus patients who do not measure blood pressure.
Goldfarb's letter added some other incredible details to the story I was unaware of including:
None of the authors of the paper have a single other co-authorship in PubMed relevant to kidney stones, other than the AHRQ review. I believe that none of the authors are nephrologists or urologists, none have a kidney stone clinic, none appear at, or present research at, kidney stone meetings, none have any experience regarding management of kidney stones
And this doozy, in response to a comment of the paper from the lead author:
As we point out in the guideline, we are aware that many physicians do select medications based on stone type, for example, allopurinol for uric acid stones, and we do not discourage that practice.
Physicians who regularly treat stones or who played NephMadness (2014 edition) know that allopurinol is used to prevent calcium stones not uric acid stones which are best treated with alkalinization.
Swapnil and I are delighted with the success of the endeavor which launched with humble beginnings on Medium aweek before the first chat with this manifesto:
Coincidental to the calendar turning over, NephJC is being recognized in two articles in the medical literature. The first is the first systematic review of microblogging journal clubs. It is an interesting and thought provoking article. NephJC takes a victory lap in Table 2:
NephJC is third in participants and total number of tweets and first in tweets and impressions per month. I found this paragraph particularly insightful:
I can't recommend the video enough. In this age where everything is sanitized and abstracted as much as possible this video is just authentic. It's as real as it gets. To me it brings to life all of the little things we ask dialysis patients to do, from waking up early, to restricting fluids, to spending 12 hours a week in a recliner hooked up to a machine with only one hand free.
I was invited to speak at the Canadian Society of Nephrology last fall. Swapnil set up a talk on social media. My first international speaking gig. Very cool.
We have two associates out on Maternity leave and another key partner retired a couple of months ago, so practice is tight. No way I could take half a week like I do for Kidney Week. I left for my 1:30 talk at 8:30 that morning. Direct flight from the D to Montreal. As I'm walking through the airport I'm looking for nephrologist ads. During Kidney Week there will always be a big a pharma company advertising in the airport. I love seeing those ads and trying to imagine wha percentage of the general population have any idea what Samsca™ or Aranesp™ are. Montreal had none of these advertisements. I took a taxi to the Hotel Bonaventure.
Found my way to the conference center and registered for the conference. The conference had about 450 people in total, about one 30th the size of Kidney Week. It is like Kidney Week Mini Me. Same clothes, same attitude but smaller. In this case a lot more than just one eighth the size.
Kidney Week is a major international conferences. I heard more foreign languages in Philadelphia last Novemebr than I heard at CSN which was being held in Montreal. We often associate size with quality but thie would be totally unfair to CSN. The lectures were amazing. They absolutly stand toe to toe with the quality you get at Kidney Week. Of course, there are some Canadian specific lectures that didn't interest me, but the general nephrology content was excellent. Five lectures in particular were amazing:
1. Patient oriented symptoms of ESRD
emolients weak data but little down side. Baby oil, primrose oil. #csn15
— Joel Topf (@kidney_boy) April 25, 2015
Uremic Pruritus: other possible txs SSRI, Ondansetron, granisetron, thalidomide, activated charcoal 6g daily. (Never duplicated) #csn15
— Joel Topf (@kidney_boy) April 25, 2015
2. Conservative care With Dr. Fliss Murtagh
Murtagh is quite prolific. Is planning an RCT to look at onservative care vs dialysis in edge cases. http://t.co/IlP4czPkKq#csn15
— Joel Topf (@kidney_boy) April 25, 2015
If your dialysis pt is/has: age >80, CHF, CAD, CVD, PVD, or BMI<19 they get all the risk of the screening and none of the benefit. #csn15
— Joel Topf (@kidney_boy) April 24, 2015
#CSN15: @NavTangri referring to a sub-group analysis on a surrogate outcome in ACCORD. Quinn looking more confident....
— Scott Brimble (@S_brimble) April 25, 2015
Con: Quinn: MDRD study primary and secondary outcomes were actually all negative. So was AASK. (proteinuria was only +ve outcome) #csn15
— Swapnil Hiremath, MD (@hswapnil) April 25, 2015
Con: Quinn demolishing AASK: if U ACHIEVE a low BP (regardless of Rx) less progression. But if U TARGET lower BP, there is no diff. #csn15
— Swapnil Hiremath, MD (@hswapnil) April 25, 2015
The plan was a one-two punch, where Sawpnil presented why you should engage with social medi,a and I followed with a "how to" engage in social media. It went well. I had some trouble using Keynote on the iPhone app to advance the slides. I used Keynote on the iPhone to control Keynote on my computer. It worked perfectly during my (admittedly abbreviated) practice sessions and for about half my presentation before it crapped out. I need a more reliable solution, please tweet recommendations. The AV-guy was pretty good at picking up my signals to advance the slides but it wasn't natural and threw my rhythm off. I'm Sorry Canada, I could've done better. That was another difference from ASN. At CSN they had no trouble wiring in my MacBook Air to their AV set-up. Much slicker than the MUST USE POWERPOINT party line from ASN.
I'll post the slides when I get a chance, but first I need to add a slide crediting @Doctor_V and Howard Rheingold, who involuntarily donated ideas to my talk. And I want to pump up the Who to Follow section with a description of mining Symplur to find thought leaders. I also need a slide telling people about Twitter4Nephrons.
In the end, I had a great time at CSN and would definitely go again; maybe not next year in Halifax, but why don't we meet the year after in British Columbia?