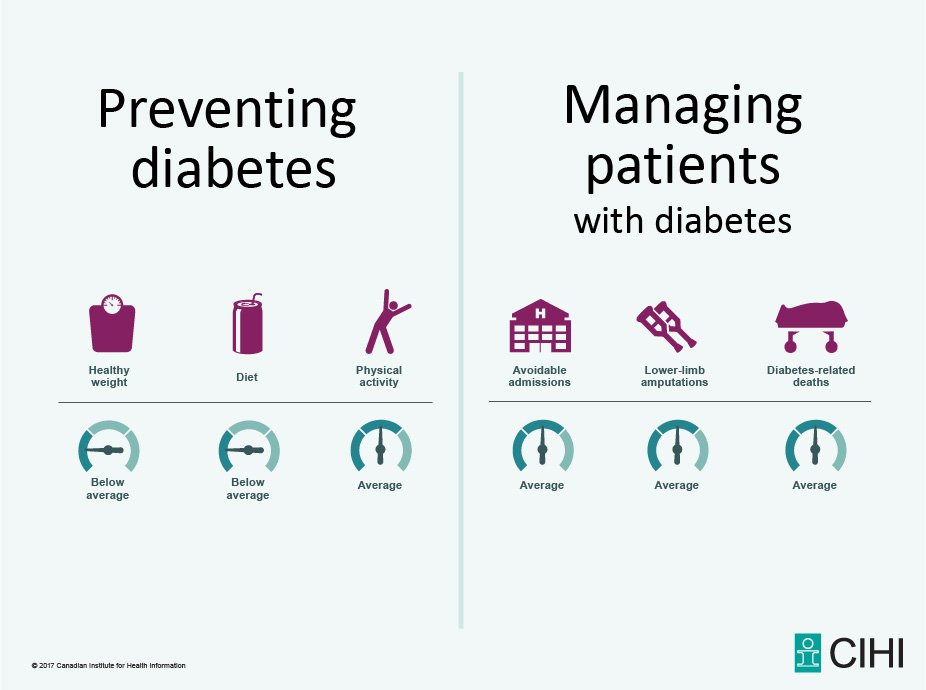
This seems like a pretty innocent infographic. It is trying to communicate how Canada is doing in preventing and managing diabetes.
Here is the tweet
Here is the response I saw in my timeline
This seemed a stretch that this poster was stigmatizing people with diabetes.
This Storify has the entire twitter exchange that follows.
I am gong to highlight a few of the tweets from that exchange here.
One of the first criticisms leveled was that the poster did not distinguish between type 1 and type 2 diabetes. This is important because the advice they were tracking and grading were all techniques to prevent type 2 diabetes: healthy weight, diet and physical activity.
This is a constant tension in building infographics, "How do you balance precision and clarity?" Not specifying type 2 diabetes makes the poster less precise but since type 2 diabetes represents 96% of diabetes in the US (not sure the Canadian data) I agree with the decision to simplify the poster. Type 1 diabetes is small potatoes compared to the public health nightmare of type 2 diabetes. Additionally, because of the potential for diabetes to grow like an epidemic and because we have tools to curtail this epidemic it becomes a good target for public health messaging in a way that type one diabetes does not lend itself.
There was then the argument that the therapy is not that effective and that people who follow this advice often still end up with diabetes:
The problem here is that since people have some agency in their disease, others will blame them for getting diabetes. The patients will be shamed because they didn't act strongly enough to avoid the disease. By publicizing ways to avoid diabetes you are setting up people with diabetes to be blamed for their condition.
How effective are the items in the poster at preventing diabetes. They are about as effective as any therapy we have in medicine. DPP is the best program to prevent diabetes.
See this RCT. What was the interventin in DPP?
The goals for the participants assigned to the intensive lifestyle intervention were to achieve and maintain a weight reduction of at least 7 percent of initial body weight through a healthy low-calorie, low-fat diet and to engage in physical activity of moderate intensity, such as brisk walking, for at least 150 minutes per week. A 16-lesson curriculum covering diet, exercise, and behavior modification was designed to help the participants achieve these goals.
All three items that are being tracked in the infographic.
So what do you get for that intervention? The
DPP trial showed
- 58% reduction in the incidence of diabetes compared to placebo.
- 39% reduction in the incidence of diabetes compared to metformin.
In 2014
1.4 million people developed type two diabetes. A 58% reduction in the incidence of diabetes means that over 800,000 people would not develop diabetes in a year.
800,000 people
That compares pretty favorably to the
total population of people with type 1 diabetes: 1.2 million.
The problem with arguing the fact that some people progress to disease despite therapy to prevent it is that none of our medications are 100% effective. If I advise patients to take their ARB because it will help their diabetes and then they develop ESRD anyways, did I invite ridicule on them because I gave them an effective therapy? Will people not provide comfort because if they had just tried harder with their ARB they would not have developed ESRD? I hope not. And that concern should not stop me from making it well known that there is an effective drug for diabetic nephropathy, it is also important to remember the treatment effect in IDNT and RENAAL were pretty modest.
 |
| Losartan reduced ESRD by 28%, but a quarter of the treated patients still ended up on dialysis by 4 years. |
 |
| Irbesartan had a similar treatment effect and a similar proportion of patients end up on dialysis despite therapy. |
We should not blame people for the diseases they develop but we should not use the fear of that blame to avoid measuring, publicizing, or developing public health initiatives, because
it looks like it maybe working.
I gave Dr. Witteman an early version of this blog post and an opportunity to respond.
Thanks for the opportunity to respond to your post. I would like to note the following five points.
- Type 1 diabetes in Canada is estimated to represent about 9% of all cases of diabetes. That's more than twice your US estimate. Even if it's still a relatively small percentage, given the prevalence of all types of diabetes, that's a lot of people. I am one of those people, so this is personally relevant to me.
- I think it's important to note that CIHI is not, strictly speaking, a public health agency. Their role in Canada is more or less to collect, collate and report data on health system quality and population health. The infographic is not intended to motivate individuals. However, when they tweet it out as they did, they're deliberately seeking a public audience.
- There is some evidence that blame & shame methods can be not only ineffective as health behaviour change mechanisms, they may be counterproductive. In other words, they may make health-related behaviours worse, not better.
- A Canadian survey in 2011 conducted on behalf of the Canadian Diabetes Association revealed that 37% of people would hesitate to tell others they have type 2 diabetes. Stigma around diabetes, particularly type 2 diabetes, is a very real issue in Canada.
- The most concerning cases of type 2 diabetes in Canada occur among people in marginalized populations (Indigenous peoples, immigrants from specific populations known to be at higher risk of type 2 diabetes, people living in poverty, etc.) Promoting the idea that diabetes is completely their own fault may reduce public support for interventions that can help prevent diabetes in these communities, including programs that promote healthy eating and physical activity. Maintaining or increasing public support for such programs is an important consideration in a publicly-funded health system such as we have in Canada.
Thank you for reaching out and offering me the opportunity to engage with you on this issue. As noted in my original 13 tweets, I strongly agree with encouraging healthy eating and physical activity. I also agree with preventing type 2 diabetes and reducing the burden that diabetes can place on people. The problem is that infographics like this typically don't move the needle, and they can even be counterproductive and harmful.
Sincerely,
Holly Witteman, PhD
.jpg)