
The benefits of RAAS inhibition in CKD are not dramatic:
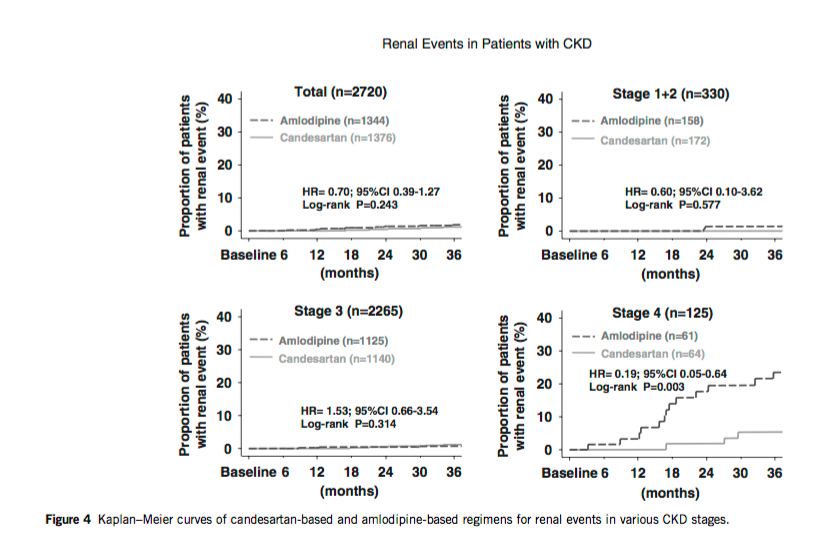
In patients with microalbuminuria, it is difficult to find any clean win. The PREVEND trial and the CASE-J trial (PDF) both showed a benefit in sub group analysis (stage 4 patients, but not in any other stages):
 |
| Renal outcomes by CKD stage (doubling of sCr, Cr>4, dialysis) |
 |
| No benefit in the whole cohort |
 |
| Anyway you cut it renal function deteriorated faster with ARB |
"The Work Group suggests ACE-Is or ARBs as the preferred class of BP-modifying agent in CKD patients with microalbuminuria. This recommendation is based on observational data and subgroup and post hoc analyses, hence the grade of 2D."On the other hand the data on macroproteinuria, even in non diabetics is not subtle:
These trials include RCTs in patients with CKD of various causes, primarily glomerulonephritis,191 African-Americans with hypertension, and patients with advanced CKD (a GFR of 20–70ml/min/1.73m2). A meta-analysis of in- dividual patient data from 11 RCTs compared antihypertensive regimens including ACE-Is to regimens without ACE-Is in 1860 patients with predominantly non-diabetic CKD. In adjusted analyses, ACE-Is were associated with a HR of 0.69 for kidney failure (95% CI 0.51–0.94) and 0.70 for the combined outcome of doubling of the baseline SCr concentration or kidney failure (95% CI 0.55–0.88). Patients with greater urinary protein excretion at baseline benefited more from ACE-I therapy (P 1⁄4 0.03 for kidney failure and P 1⁄4 0.001 for the combined outcome).Here are some of the key figures from the above mentioned meta-analysis (11 studies, 1,860 non-diabetic patients, RCT ACE-i vs non-ACEi) from Annals of Internal medicine:
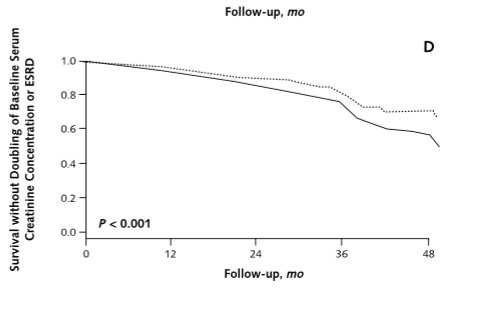 |
| Those lines are diverging over time. Right? |
 |
| Looks like a solid RR of 0.6 to 0.7 with ACEi |
 |
| The higher the proteinuria the greater the benefit. |
 The NNT to prevent the composite end-point of ESRD or doubling of serum creatinine is a robust 14!
The NNT to prevent the composite end-point of ESRD or doubling of serum creatinine is a robust 14!Of note from this study 4% of patients were withdrawn due to ACEi side effects, which included the dreaded hyperkalemia.

But the question that I have; the question that nags at me, is, "Are the patients that live at the left end of the bell curve, the ones that were unable to tolerate the ACEi due to hyperkalemia, do they have the same physiology and neurohormonal milieu as the rest of the cohort? Could those patients have naturally low angiotensin 2 levels or low aldosterone levels?" It seems likely.

And if that is the case, it also seems more likely that these patients would be among the 13 patients in our NNT of 14 that do not benefit by not doubling their creatinine or going on dialysis. It's like their bodies have endogenous RAAS inhibition.

If that is the case, that these patients do not benefit from RAAS inhibition then they are not harmed by stopping the drug and hence they would not get a benefit from patiromer.
The essential issue is that though we have shown a benefit of RAAS inhibition for renal outcomes in CKD, we have never shown that benefit in patients who could not tolerate the drug and I think the sliver of patients who cannot tolerate RAAS inhibition may represent a population different enough from the whole cohort to deserve study.
I plan on using patiromer in my patients but it is hard to be a cheer leader for the drug or feel that it is an essential part of the treatment regiment until we see the benefit in this targeted population.
--UPDATE--
So I received this tweet from David Goldfarb
@kidney_boy what about possibility that hyperK on RAASi means that RAAS is MORE activated? that rise in K is assay for effective drug?
— David S Goldfarb (@weddellite) February 1, 2016
I replied:
@weddellite has anybody done TTKG before and after ACEi and correlated it with clinical outcomes? Does ↓ TTKG ☞ improved outcomes?
— Joel Topf (@kidney_boy) February 1, 2016
Then I entered the following search:


My search criteria was almost a perfect match for the title of the article. The article shows worse outcomes for patients with increased serum potassium but it did not separate out people by the change in serum potassium or look at renal potassium handling, both of which would be ideal. But that said, there is no signal that increased potassium is a harbinger of increased benefit from ARBs.
Take a look at the response too.

{kind=link}
{kind=link}