283 posts with another 24 drafts that have not yet seen the light of day.
283 posts in 730 days is one post every two and a half days. Not bad.


After three glasses of wine he felt as though he had a bottle and a half, with memory loss.The only other paper I could find was by McDowell, Chittick, et al. who looked at increased abacavir levels with alcohol intake. The reverse of what I was looking for, but at least it was related. They gave a single dose of abacavir and 0.7 g/kg of ethyl alcohol to 25 HIV positive men. They found a 26% increase in the half life of abacavir with alcohol but...
This study did not demonstrate any alteration in the pharmacokinetic parameters of ethanol by abacavir coadministration; blood ethanol median profiles following ethanol administration in the presence and absence of abacavir were essentially superimposable. There was no evidence that co-administration of abacavir interferes with ethanol metabolism. There were no disulfiram-type reactions in any subject who received coadministration of abacavir and ethanol.This study tested the effects of a single dose of abacavir, chronic dosing may result in a different effect on alcohol dehydrogenase.
Anonymous said...
Why wait one entire year to correct the Deficiency. I would have treated with 100,000 units po qd for 5-10 days.
I responded...
Regarding the time to treat the patient. This patient had almost no appreciable renal disease outside of the SHPTH. I was not going to schedule frequent visits to monitor therapy I just put them on a safe and familiar vitamin D dose and followed up every six months. I don't think I harmed the patient with slow therapy. The one time I had a patient on 50,000 units daily (resident error) they were readmitted within 2 weeks with hypercalcemia.


But come on, are sodas really so bad? Even coffee drinkers like to use a little sugar. Should we demonize coffee, too? Well, as a thought experiment, imagine that you're in the office kitchen as a colleague adds some sugar to his coffee. As you watch, he adds a teaspoon. And then another. And another. And another. And another. And another. And another.And another. And another. And another. And another. And another. And another. And another. And another. And another. (Dude, want some coffee with your sugar?)



The likelihood of renal replacement therapy, either transplant or dialysis, was near zero (≤1.3%) for patients in all stages except stage 4, where 2.3% ± 1.1% of patients received a transplant and 17.6% ± 2.7% had dialysis initiated.




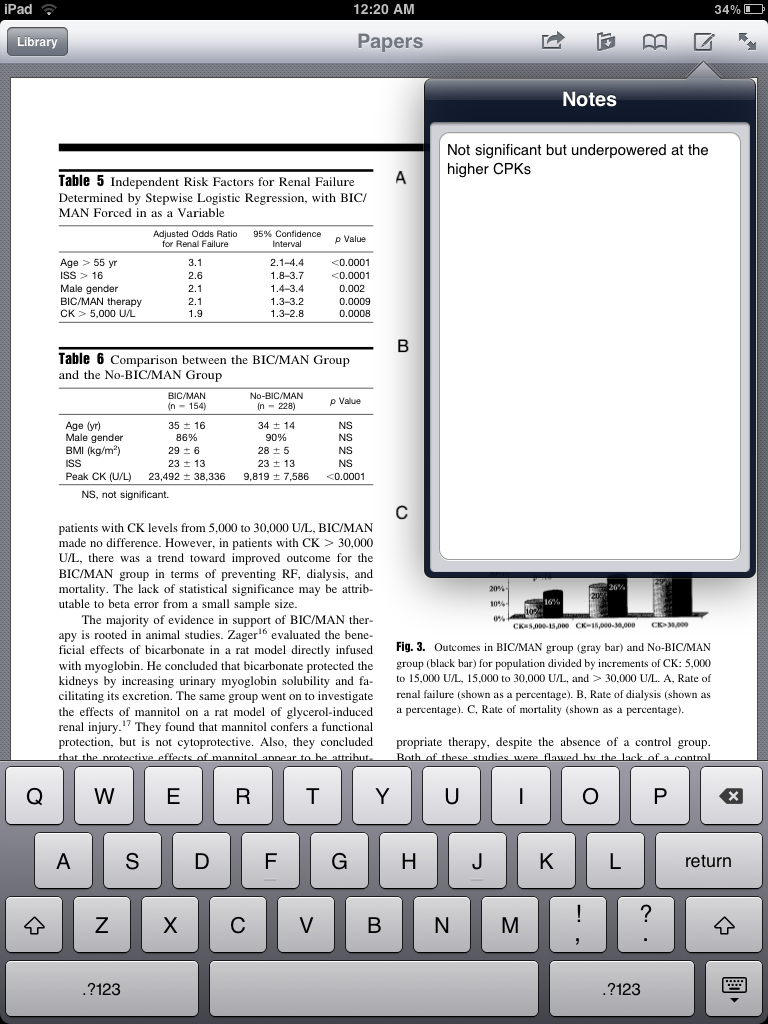
In a large series of 382 patients with serum CK concentration >5000 U/L, 154 (40 percent) were treated with bicarbonate and mannitol [33]. There was no statistically significant difference in the incidence of renal failure (creatinine >2.0 mg/dL [177 micromol/L]; 22 versus 18 percent), dialysis (7 versus 6 percent), or death (15 versus 18 percent) in patients who were or were not treated with bicarbonate and mannitol. However, there was a trend toward improved outcomes in patients with extremely high CK levels (>30,000 U/L) treated with bicarbonate and mannitol.Reference 33 is the primary reference for one of my first blog posts. We started talking about this study on rounds, but the crap machines in the ICU didn't have Flash or PDF support. I ended up downloading the PDF on my iPhone and four of us passed it around to look at some of the figures. The iPad doesn't have flash but it does a beautiful job rendering PDFs. I have the article in Papers which does an awesome job at holding and organizing my entire medical library.
 Papers is iTunes for scientific Papers. It is the modern equivalent to the file cabinet you always wanted for all the important scientific articles that fall into your grubby little hands. My computer is littered with literally hundreds of scientific articles. What you want to do is throw them all into Papers.
Papers is iTunes for scientific Papers. It is the modern equivalent to the file cabinet you always wanted for all the important scientific articles that fall into your grubby little hands. My computer is littered with literally hundreds of scientific articles. What you want to do is throw them all into Papers.










 In 2002 at the Spring Clinical Meeting of the National Kidney Foundation, K/DOQI released the Clinical Practice Guidelines for Chronic Kidney Disease Evaluation, Classification and Stratification.
In 2002 at the Spring Clinical Meeting of the National Kidney Foundation, K/DOQI released the Clinical Practice Guidelines for Chronic Kidney Disease Evaluation, Classification and Stratification.GFR=186 x sCr -1.154 x Age -0.203 x (0.742 if female) x (1.212 African-American)African Americans, for the same creatinine, are given a 21% increase in their GFR and women lose 26%. If GFR provided prognostic information one would think that African Americans were protected from chronic kidney disease and women were at higher risk. Yet that is not the case. African Americans have the highest rates of ESRD, 998 per million compared to 273 for white Americans: (USRDS 2009 Annual Data Reports, NIH, NIDDK, Bethesda, MD, 2009.)





