Membranous nephropathy is a common finding when patients are biopsied for nephrotic syndrome. Fortunately, it is a relatively benign disease with a significant number of spontaneous remissions. (Schieppati, NEJM 1993)

Adequate renal function was defined as "no ESRD"

Since there are so many spontaneous remissions and the therapy has significant side-effects we risk stratify patients in order to spare low-risk patients from treatment.
Higher risk
- older age (over 60) (Medline)
- male sex
- nephrotic range proteinuria
- greater than 8-10 g/day for more than 6 months (PDF)
- increased serum creatinine (Cr over 1.5) (Medline)
Though the instinct after getting a kidney biopsy is to start therapy immediately, in patients with a normal creatinine, waiting for 6 months and monitoring the creatinine and proteinuria does not alter the patients response to treatment. (Medline)
The biopsy findings have long been held of major importance on predicting prognosis but an analysis of 389 biopsies questioned whether histology provided information that independently predicted prognosis. (Medline)
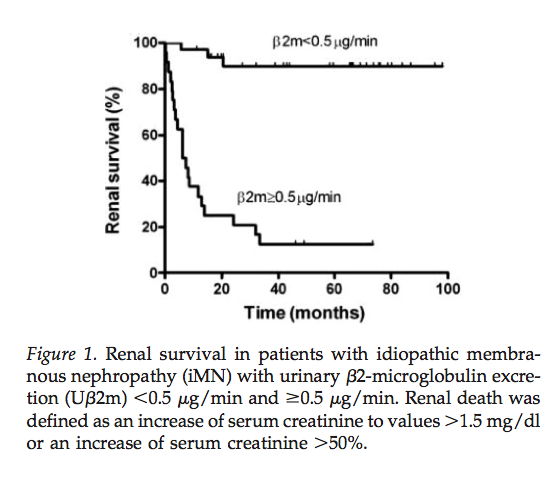
Two urinary findings are gaining acceptance at being able to better predict the clinical course of disease. Beta-2 microglobulin excretion greater than 0.5 mcg/min and IgG excretion over 250 mg per day (others use the more sesitive value of 125 mg/24 hours) have both been associated with increased risk of renal progression. (Medline)


Treatment
The biopsy findings have long been held of major importance on predicting prognosis but an analysis of 389 biopsies questioned whether histology provided information that independently predicted prognosis. (Medline)
Two urinary findings are gaining acceptance at being able to better predict the clinical course of disease. Beta-2 microglobulin excretion greater than 0.5 mcg/min and IgG excretion over 250 mg per day (others use the more sesitive value of 125 mg/24 hours) have both been associated with increased risk of renal progression. (Medline)

Treatment
Treatment recomendations are based on the probability of progression.
Low Risk
For patients with a low risk of progressing the recommendation is to stay and pray.
- Monitor the creatinine
- Institute non-specific antiproteinuric therapy (ACEi, ARB, aldosterone antagonists)
- Control the lipids
- Tight blood pressure control
Moderate risk
 These patient should be initiaed on the Ponticelli or modified Ponticelli protocol. This calls for three consecutive two-month cycles of cytotoxic therapy.
These patient should be initiaed on the Ponticelli or modified Ponticelli protocol. This calls for three consecutive two-month cycles of cytotoxic therapy.- Day 1-3: 1 gram of methylprednisolone. This is usually done as an inpatient.
- Day 4-30: Oral prednisone, 0.5 mg/kg daily
- Day 31-60: Oral cyclophosphamide 2 mg/kg (chlorambucil in the original Ponticelli)
High risk
Less data is available. Modified Ponticelli maybe appropriate but others recommend cyclosporin.
For patients with resistant disease there is no consensus on what is best and a list of what's been tried looks like a line up of the usual suspects, nephrology edition.
