Sunday, March 23, 2014
Alternative Medicine in U.S. Medical Schools
Nice lecture that dove tails with my herbal toxin lecture.
Friday, March 21, 2014
NRMP Crack
I just heard about this yesterday and loved the irony. The NRMP which toys with the emotions of med students everywhere by holding back match results until that wonderfully cinematic moment on Match Day, accidently leaked the match results. Shoddy programming.
Here is the thread from redddit.
Here is a blog post about the slip up:
Happy Match Day. Good luck and "...may the odds be ever in your favor."
Here is the thread from redddit.
Here is a blog post about the slip up:
As you can imagine, this created QUITE a stir, as medical students around the country have been waiting, stressed out of their minds, about where they will be assigned to go to residency for the next 4-7 years. A flurry of online activity ensued, as medical students already pushed to the brink took to their browser’s source codes to figure out their futures. Apparently the programmers “preloaded” the match homepage source code with the information of where people match, so that once the magic time hits on Friday, they can easily change everyone’s NRMP homepages to reveal the new result. What they didn’t realize? That there are medical students out there who are combing every detail of the site to figure out anything they can ahead of time. Several took it upon themselves to poll all of their friends to assess the accuracy of this method.So today's match day will have a little less drama, for every fourth year who was not obsessing over the match results.
Happy Match Day. Good luck and "...may the odds be ever in your favor."
NephMadness. The story behind the brackets.
Last year, NephMadness came together in about 4 weeks from concept to Selection Sunday. Because of the short time available, and the fact that we had no idea what we were doing, somethings worked and others flailed. Since we are in the middle of a bracket fever epidemic, let's take a critical look at last year's brackets with a focus on the changes we made in 2014.

The most important thing we got right, was dividing the field into 8 regions of 8 teams and assigning unique themes to each of these regions. In 2013 the 8 themes were:


An example of this working to perfection was in Kidney Stones.

David Goldfarb, immediately grokked the game and over the course of an hour long phone call filled his brackets with great pairings that hit on stone issues relevant to nephrologists. He selected teams that represented diagnosis, treatment, the future and the past. He built a bracket that we, literally, could not have done without him.
The most important thing we got right, was dividing the field into 8 regions of 8 teams and assigning unique themes to each of these regions. In 2013 the 8 themes were:
- Big organized programs like Medicare ESRD benefit and USRDS
- Research techniques like randomized controlled trials, propensity scoring and epigenetics
- Randomized clinical trial like TREAT, IDEAL and ALLHAT
- Molecules and genes, think FGF23, Cystatin C, APOL1
- Drugs like captopril, cyclosporin and tolvaptan
- Educational resources like UpToDate, Renal Fellow Network and Wikipedia (yeah, we went there)
- Equations we use Winter's formula, MDRD, FENa
- Renal procedures like kidney biopsy, scribner shunt and plasmapheresis.
This provided a degree of rationality to an inherently irrational game. Where we fell down is when we didn't adhere to the themes. Look at the molecules and genes region, somehow MPGN reclassification and HIVAN slipped in.
Likewise in the procedures section we had an eclectic group that included completely disjointed procedures such as transplant, citrate anticoagulation and the Scribner shunt.
The other primary weakness of the 2013 field was that there were a few overwhelming stands outs. Just glancing at the tournament a few Goliaths stood out that you just knew were going to end up in the final four. Here was our final four from last year:
- Captopril (1)
- Medicare ESRD benefit (1)
- HEMO trial (1)
- Transplant (2)
Three number one seeds and a number two seed. Looking over this year's brackets, I don't see obvious candidates for the final four.
When we started thinking about assembling the field for 2014, we decided to get outside help. The plan was to work with experts in various corners of nephrology to unearth some gems that the core editors of NephMadness would never have considered.
When we started thinking about assembling the field for 2014, we decided to get outside help. The plan was to work with experts in various corners of nephrology to unearth some gems that the core editors of NephMadness would never have considered.
An example of this working to perfection was in Kidney Stones.
David Goldfarb, immediately grokked the game and over the course of an hour long phone call filled his brackets with great pairings that hit on stone issues relevant to nephrologists. He selected teams that represented diagnosis, treatment, the future and the past. He built a bracket that we, literally, could not have done without him.
It has been great, getting a chance to correct the mistakes of version of 1.0 to build something of quality. I have to say that the most rewarding part of NephMadness was putting together the selection committee and talking with them about their area of expertise. Just letting an expert who has spent her whole life studying one corner of nephrology expound on what is so important and exciting about that field was super enjoyable. (Unless, they didn't get NephMadness, and in that case it was more like a root canal)
The NCAA tournament has started but you can still join NephMadness. Get in the game before Wednesday, March 26th.
Tuesday, March 18, 2014
Dialysis for toxic alcohols, new empiric data
Why I love twitter.
Immediate download.
Interesting introduction in the article about the disparity betweeen cases and resources for treating methanol. Most resources are available in the developed world (dialysis, fomepizole) but most cases occur in the developing world. Also interesting note was that some Islamic Countries have social bans on the medicinal use of alcohol. That could make treatment pretty dicey.
They prospectively observed 24 cases of methanol ingestion out of 121 cases in a mass methanol poisoning in the Czech Republic. Looks like it was due to contamination of spirits with industrial methanol. Apparently this is a relatively common problem.
41 deaths. All patients in the observation cohort were treated with ethanol (17 patients) or fomepizole (4) or both (3) to prevent conversion of methanol to the downstream toxic metabolite, formic acid.
The authors present clearance data on 11 patients treated with conventional dialysis and 13 treated with continuous dialysis.
The half life of methanol with conventional dialysis was 3.7 hours and 8.1 hours with continuous dialysis. Not suprisingly all of the componants associated with more efficient dialysis were associated with with faster clearance of methanol: increased dialyzer surface area, increased blood flow and increased dialysate flow. Those half-lifes are remarkably shorter than the half life of methanol in the body using renal and pulmonary clearance.
On the other hand folate supplementation, the pre-dialysis methanol level and the nature of the antidote (ethanol versus fomepazole) made no difference.
The shorter half-life with intermittent conventional dialysis did not transplant into better patient survival.
They turned their math into specific treatment guidelines.

Some interesting tidbits. You know that graft that shows that the osmolar gap falls as the anion gap rises?
That wasn't the case so much here, they found simultaneous high anion and osmolar gaps.

Intermittent HD superior to CVVHD in removing methanol and formate in methanol poisoning. http://t.co/8sHi23RnLu cc: @kidney_boy
— Bryan D. Hayes (@PharmERToxGuy) March 17, 2014
Immediate download.
 |
| See if you can get a few more authors next time. |
They prospectively observed 24 cases of methanol ingestion out of 121 cases in a mass methanol poisoning in the Czech Republic. Looks like it was due to contamination of spirits with industrial methanol. Apparently this is a relatively common problem.
41 deaths. All patients in the observation cohort were treated with ethanol (17 patients) or fomepizole (4) or both (3) to prevent conversion of methanol to the downstream toxic metabolite, formic acid.
 |
| 15 years old and this page still stands-up. Some stuff never changes. Page 358 of the Fluids Book. . |
The half life of methanol with conventional dialysis was 3.7 hours and 8.1 hours with continuous dialysis. Not suprisingly all of the componants associated with more efficient dialysis were associated with with faster clearance of methanol: increased dialyzer surface area, increased blood flow and increased dialysate flow. Those half-lifes are remarkably shorter than the half life of methanol in the body using renal and pulmonary clearance.
On the other hand folate supplementation, the pre-dialysis methanol level and the nature of the antidote (ethanol versus fomepazole) made no difference.
The shorter half-life with intermittent conventional dialysis did not transplant into better patient survival.
They turned their math into specific treatment guidelines.
Some interesting tidbits. You know that graft that shows that the osmolar gap falls as the anion gap rises?
 |
| Canadian Family Physician |
Saturday, March 15, 2014
My post for World Kidney Day
Things a re a bit frantic with the start of NephMadness just over 24 hours away.
I'm going to be doing more and more of my posts on Medium, it is so much better than WordPress or Blogger for composing and displaying my words.
Sitting on the flight deck of #NephMadness One. Note the glom pic the wife got me for Valentines day! pic.twitter.com/iMLgTlidQR
— Joel Topf (@kidney_boy) March 12, 2014
I posted on World Kidney Day at Medium but I failed to link to on PBFuids. Sorry. |
| My very optimistic post for WKD |
I'm going to be doing more and more of my posts on Medium, it is so much better than WordPress or Blogger for composing and displaying my words.
Monday, March 10, 2014
Follow-up from the Herbal Supplements Lecture
I received a delightful e-mail from Arthur Grollman, world expert on Aroistocholic Acid.
Dear Dr Topf,
I congratulate you on assembling and sharing this very nice presentation and, wisely, connecting it to the problems associated with politicians, supplements and DSHEA. We have written some articles about this connection as well.
I give a similar lecture to medical students and another focussed on BEN [ed: Balkan Endemic nephropathy] and aristolochic acid nephropathy for Medical and Nephrology Grand Rounds as most of the research being done on that subject since 2005 has been done in our lab.
A few comments on the historical sequence:
We continue to work on this fascinating nephrotoxin/carcinogen for which, as you see has a "signature mutation" and is likely to affect tens of millions of people in China. And the road to its recognition started exactly as you said in your talk, with the two
- JP Cosyns is the Belgian pathologist who first recognized the similarity to BEN but did not follow up the lead
- Tjassa Hranjec, a medical student at Stony Brook, doing a summer fellowship conducted the personal interview with the farmer you attributed to me. She
- was doing a pilot epi study, under my direction, to determine how we should investigate BEN
- The first experimental evidence for the role of AA in AAN and UTUC appears in our 2007 PNAS paper
- The Serbs and the Bosnians still believed that their BEN was a different disease, so we expanded the number of cases and included those countries in the cover story paper in KI in 2012. DeBroe wrote a commentary to accompany our paper which convinced any remaining skeptics of the validity of our guiding hypothesis: AAN = CHN = BEN
- Wondering how Aristolochia herbs could have been used throughout the world for 2000 years without one mention of toxicity or urothelial cancer, we conducted the study in Taiwan, where one in three people have ingested the Aristolochia herb according to the prescription database. The results are in our 2012 PNAS paper.
Belgian women in Vanderwegen's clinic. He told me that his own clue came when he walked from his office to the clinic and found a number of women talking to each other which was unusual. He asked them how they knew each other which led immediately to the identification of the spa.
With best regards
Arthur P. Grollman M.D.
Distinguished Professor of Pharmacological Sciences
Evelyn Glick Professor of Experimental Medicine
Director: Laboratory of Chemical Biology
Health Sciences Center BST-8-160
Stony Brook University

 |
| Gorgeous picture of DNA Adducts |
Grollman won the 2011 Environmental Mutagen Society Award. As part of that award he wrote an invited review on aristocholic acid nephropathy. I'm looking forward to reading it. It has some great drawings. Take a look at the figure below the abstract. Wow.


He included this reading list for people interested in the connection illustrated above:
- Aristolochic acid-associated urothelial cancer in Taiwan
- Aristolochic acid and the etiology of endemic (Balkan) nephropathy (full text)
- Chinese herbs nephropathy and Balkan endemic nephropathy: toward a single entity, aristolochic acid nephropathy
- Aristolactam-DNA adducts are a biomarker of environmental exposure to aristolochic acid (full text)
Friday, March 7, 2014

Tuesday, March 4, 2014
#DreamRCT: The final push
The DreamRCT project launched just over a month ago on January 28th.  It has exciting seeing people across the nephrology blogosphere participate in this project. But all good things need to wrap-up. NephMadness is approaching so it is time for everyone to rank their favorite post.
It has exciting seeing people across the nephrology blogosphere participate in this project. But all good things need to wrap-up. NephMadness is approaching so it is time for everyone to rank their favorite post.
Go to UKidney to view and rank your favorite DreamRCTs
The voting is currently neck and neck, help push your favorite over the top! And if you have a great idea for a DreamRCT, get in quick, the doors are still open. Having trouble coming up with an idea, how about pone of these:
It has exciting seeing people across the nephrology blogosphere participate in this project. But all good things need to wrap-up. NephMadness is approaching so it is time for everyone to rank their favorite post.Go to UKidney to view and rank your favorite DreamRCTs
The voting is currently neck and neck, help push your favorite over the top! And if you have a great idea for a DreamRCT, get in quick, the doors are still open. Having trouble coming up with an idea, how about pone of these:
- Systolic blood pressure targets in proteinuric disease less than 140 vs less than 130. Fill in the hole left from ACCORD BP.
- Fixed ESA dose vs pharmacodynamic dosing (current standard of care). This editorial gets at some of the issues I'd like to explore, but doesn't fully flesh it out.
- PTH liberal strategy vs conservative PTH strategy. Randomize patients to get PTH lowering therapy based on target PTHs, current standard of care versus only intervene for symptoms such as bone pain and itching. Answer once and for all, is PTH important?
I have one more idea for a totally crazy DreamRCT that I will try to submit in the next few days.
Monday, March 3, 2014
Lecture on Herbal Medicine and Kidney Disease
In August of 2013, I went to Chicago for the ASN Board Review Class. The week long class was filled with great lectures and compelling teachers, but it was a review and I had solid knowledge of most sessions, but one session was different. Warren Kupin (Hey, Warren, we are still waiting for your first tweet!) of the University of Miami gave an inspired lecture on interstitial nephritis and the dangers of herbal medications. It was one of the most interesting lectures I have ever seen and I decided that I would remix his lecture for my February grand rounds.
I gave this grand rounds at St Johns and Providence Hospital last week (two grand rounds, same subject, same week, that's lecturing like a boss).
Here is a link to see the presentation with me narrating.
Same presentation but higher quality.
The original Keynote file is available here for remixing and editing.
A PDF of the presentation is available here.
 Much of the information on sulfanilamide comes from this article by the FDA.
Much of the information on sulfanilamide comes from this article by the FDA.
 The picture comes from an ad on Etsy. I didn't get permission to use the photo, but I did buy the bottle, so that should be cool.
The picture comes from an ad on Etsy. I didn't get permission to use the photo, but I did buy the bottle, so that should be cool.
 Harold Watkins committed suicide after the sulfonilamide disaster, though the owner of the Messengill Company never showed any regrets: Dr. Samual Evans Massengill, the firm's owner, said: "My chemists and I deeply regret the fatal results, but there was no error in the manufacture of the product. We have been supplying a legitimate professional demand and not once could have foreseen the unlooked-for results. I do not feel that there was any responsibility on our part."
Harold Watkins committed suicide after the sulfonilamide disaster, though the owner of the Messengill Company never showed any regrets: Dr. Samual Evans Massengill, the firm's owner, said: "My chemists and I deeply regret the fatal results, but there was no error in the manufacture of the product. We have been supplying a legitimate professional demand and not once could have foreseen the unlooked-for results. I do not feel that there was any responsibility on our part."
 Diethylene glycol, though it contains two molecules of ethylene glycol there is no evidence that it behaves like ethylene glycol in a poisonong and no evidence that fomepizole would be protective. Contemporary experience with diethylene glycol comes from the Haiti Contamination disaster and a PDF from JAMA.
Diethylene glycol, though it contains two molecules of ethylene glycol there is no evidence that it behaves like ethylene glycol in a poisonong and no evidence that fomepizole would be protective. Contemporary experience with diethylene glycol comes from the Haiti Contamination disaster and a PDF from JAMA.
 There are various reports for how much was shipped and how much was confiscated, I took one set of data and ran with it. If I'm wrong, shoot me.
There are various reports for how much was shipped and how much was confiscated, I took one set of data and ran with it. If I'm wrong, shoot me.
 The Kelsey information is almost entirely from Wikipedia.
The Kelsey information is almost entirely from Wikipedia.
 Getting reliable data on the size of the herbal supplement business was nearly impossible, I found sources that used anywhere from 5 billion to 100 billion. Most sources were around 26 billion so that is what I used. I imagine it depends a lot on what you includein dietary supplements and herbal medication. Of note, GNC alone does 2.6 billion dollars in revenue.
Getting reliable data on the size of the herbal supplement business was nearly impossible, I found sources that used anywhere from 5 billion to 100 billion. Most sources were around 26 billion so that is what I used. I imagine it depends a lot on what you includein dietary supplements and herbal medication. Of note, GNC alone does 2.6 billion dollars in revenue.
 I like this slide, but it doesn't really fit into the lecture. I bet it gets cut in a future presentation.
I like this slide, but it doesn't really fit into the lecture. I bet it gets cut in a future presentation.
 The tag line that people take the drugs for years, what they may take changes but they will take something for years, comes almost verbatem from Kupin's lecture.
The tag line that people take the drugs for years, what they may take changes but they will take something for years, comes almost verbatem from Kupin's lecture.


I really like the chart styles I used in this lecture. One of the problems with pie graphs is trying to associate a color to a trend. what part of the pie is attached to what is happening. By making one color with maximum contrast and the other with no contrast (transparent), it becomes much clearer. If I were to change anything I would get rid of the title of the slide and increase the typeface over the pies. Kupin's slide with the same data for comparison.
The silicate stone story is a little weak and could be cut.

Love this slide. Kupin's idea to leverage physician familiarity with Grapefruit interactions with how St. John Wort interacts. He is really clever.
 The Metabolife story is so good it should be made into a movie. And the only reason there is an anvil animation is so you can drop the bars over some guy. Love this slide.
The Metabolife story is so good it should be made into a movie. And the only reason there is an anvil animation is so you can drop the bars over some guy. Love this slide.
 The Seville Orange and synephrine works great. The Blue Cohosh data is a little light and the fact that there aren't a million weight loss agents using it makes me suspect that it is not a very powerful alpha agonist. May need to research this herb more thoroughly.
The Seville Orange and synephrine works great. The Blue Cohosh data is a little light and the fact that there aren't a million weight loss agents using it makes me suspect that it is not a very powerful alpha agonist. May need to research this herb more thoroughly.
 I need to include the incredible aspect that Patrick Arnold was the guy who brought DMAA back from the dead. Patrick Arnold was the chemist behind BALCO and inventor of The Clear.
I need to include the incredible aspect that Patrick Arnold was the guy who brought DMAA back from the dead. Patrick Arnold was the chemist behind BALCO and inventor of The Clear.
 Wife helped me with this slide, the first version had patient temperatures and ambient temperatures on a single thermometer.
Wife helped me with this slide, the first version had patient temperatures and ambient temperatures on a single thermometer.
 The Cheerios story is cute, and illustrative but it could be sacrificed.
The Cheerios story is cute, and illustrative but it could be sacrificed.
 One of the funniest parts of Kupin's talk is when he goes off on the crazy ridiculous packaging of herbal medications (American products waving the Dutch flag, etc.). I couldn't pull it off and added this single slide. I may talk a bit more about the packaging requirements of DSHEA.
One of the funniest parts of Kupin's talk is when he goes off on the crazy ridiculous packaging of herbal medications (American products waving the Dutch flag, etc.). I couldn't pull it off and added this single slide. I may talk a bit more about the packaging requirements of DSHEA.
 This slide worked as well as I hoped it would. Big risk talking about erections for a slide with 43 builds. It worked.
This slide worked as well as I hoped it would. Big risk talking about erections for a slide with 43 builds. It worked.
 Weight loss supplements, go home, you're drunk.
Weight loss supplements, go home, you're drunk.
Phenolphthalein. Really?
 The Glycyrrhiza glabra joke? It's Kupin's. The guy is really funny.
The Glycyrrhiza glabra joke? It's Kupin's. The guy is really funny.
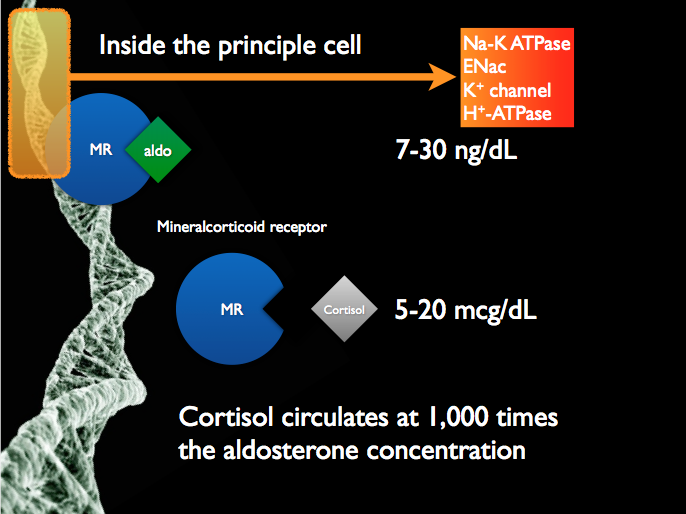 The 11beta-hydroxysteroid dehydrogenase story comes from my metabolic alkalosis, potassium and monogenic hypertension lecture.
The 11beta-hydroxysteroid dehydrogenase story comes from my metabolic alkalosis, potassium and monogenic hypertension lecture.
 Love this twist to the Aruvedic medicine study. I find it so funny, it is the kind of thing that usually doesn't make it into the methods. #OverlyHonestMethods
Love this twist to the Aruvedic medicine study. I find it so funny, it is the kind of thing that usually doesn't make it into the methods. #OverlyHonestMethods
 Kupin spent a lot of time in his lecture talking about this. I blew through it pretty quickly. I may make time for this in a future version.
Kupin spent a lot of time in his lecture talking about this. I blew through it pretty quickly. I may make time for this in a future version.
 Love the way I told the Aristolochic Acid story. And this story board where I select the different countries turned out just like I hoped it would.
Love the way I told the Aristolochic Acid story. And this story board where I select the different countries turned out just like I hoped it would.
 The most important slides in the deck?
The most important slides in the deck?
 This slide didn't work as well as I would like.
This slide didn't work as well as I would like.
The next version should add some of the data I started to put together on vitamins, especially the SELECT trial and the USPTF statement saying that vitamins have no role in the prevention of cancer of cardiac disease.
I gave this grand rounds at St Johns and Providence Hospital last week (two grand rounds, same subject, same week, that's lecturing like a boss).
Here is a link to see the presentation with me narrating.
Same presentation but higher quality.
The original Keynote file is available here for remixing and editing.
A PDF of the presentation is available here.
Notes on the presentation
@kidney_boy One (minor) thing - McGill University is in Montreal, not Toronto. Can get folks upset here in Canada. :) (McGill grad here)
— Michelle Gibson (@MCG_MedEd) March 4, 2014
I really like the chart styles I used in this lecture. One of the problems with pie graphs is trying to associate a color to a trend. what part of the pie is attached to what is happening. By making one color with maximum contrast and the other with no contrast (transparent), it becomes much clearer. If I were to change anything I would get rid of the title of the slide and increase the typeface over the pies. Kupin's slide with the same data for comparison.
The silicate stone story is a little weak and could be cut.
Love this slide. Kupin's idea to leverage physician familiarity with Grapefruit interactions with how St. John Wort interacts. He is really clever.
Phenolphthalein. Really?
It's principal cell not principle cell. Thanks Matt.
The next version should add some of the data I started to put together on vitamins, especially the SELECT trial and the USPTF statement saying that vitamins have no role in the prevention of cancer of cardiac disease.
Subscribe to:
Comments (Atom)
